Congratulations on taking your first step to
a good night's sleep without a CPAP.
A sleep specialist will be with you shortly...

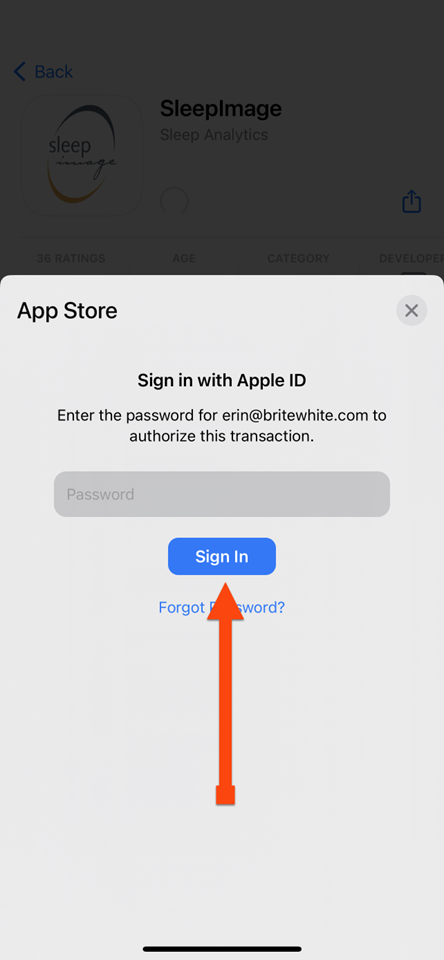
LOGIN

WHAT PROMPTED YOU TO CONTACT US?
HOW'S SLEEPING WITH YOUR CPAP?

Discreet & Quiet
Cleaning is Simple
Traveling is Light
Camping is a Breeze
NORMAL BREATHING
SLEEP APNEA BREATHING
HOW A CPAP WORKS
HOW A SLEEP APPLIANCE WORKS
5 EASY STEPS TO TREATING SLEEP APNEA AND REPLACING YOUR CPAP
5 EASY STEPS TO TREATING SLEEP APNEA AND REPLACING YOUR CPAP
5 EASY STEPS TO TREATING SLEEP APNEA AND REPLACING YOUR CPAP
5 EASY STEPS TO TREATING SLEEP APNEA AND REPLACING YOUR CPAP
5 EASY STEPS TO TREATING SLEEP APNEA AND REPLACING YOUR CPAP
ACCOMPLISHED IN THE COMFORT OF YOUR HOME

YOUR PERSONAL INFORMATION
First and Last Name?

YOUR PERSONAL INFORMATION
Name:
Is your name spelled correct?
YOUR PERSONAL INFORMATION
Address?
YOUR PERSONAL INFORMATION
Address:
,
Is your address correct?
YOUR PERSONAL INFORMATION
Cell Number?

YOUR PERSONAL INFORMATION
Cell Number:
Is your cell number correct?
YOUR PERSONAL INFORMATION
Phone Number?

YOUR PERSONAL INFORMATION
Phone Number:
Is your phone number correct?
YOUR PERSONAL INFORMATION
Email Address?

YOUR PERSONAL INFORMATION
Email:
Is your email correct?
YOUR PERSONAL INFORMATION
Gender?

YOUR PERSONAL INFORMATION
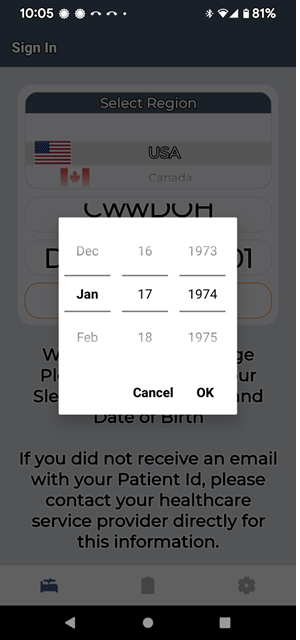
Date of Birth?

YOUR PERSONAL INFORMATION
Is your date of birth correct?
Date of Birth:
TIME ZONE
What time zone?

YOUR PERSONAL INFORMATION
Is your time zone correct?
Your Time Zone:
DO YOU HAVE DENTURES?

YOUR MEDICAL INFORMATION
Do you have Medicaid?
YOUR INSURANCE INFORMATION
Medicare?
Medicare Replacement?
Medical Insurance?

YOUR INSURANCE INFORMATION
Name of Insurance?

YOUR INSURANCE INFORMATION
Is the insurance name correct?
Name of Insurance:
YOUR INSURANCE INFORMATION
Claims Address?

YOUR INSURANCE INFORMATION
Is the claim address correct?
Claim Address:
, -
YOUR INSURANCE INFORMATION
Claim's Phone Number?

YOUR INSURANCE INFORMATION
Is the claim's phone number correct?
Claim's Phone Number:
YOUR INSURANCE INFORMATION
Claim's Fax Number?

YOUR INSURANCE INFORMATION
Is the claim's fax number correct?
Claim's Fax Number:
YOUR INSURANCE INFORMATION
Subscriber ID?

YOUR INSURANCE INFORMATION
Is the subscriber id correct?
Subscriber ID:
YOUR INSURANCE INFORMATION
Subscriber Name?

YOUR INSURANCE INFORMATION
Is the subscriber's name correct?
Subscriber Name:
YOUR INSURANCE INFORMATION
Subscriber Date of Birth?

YOUR INSURANCE INFORMATION
Is the subscriber's date of birth correct?
Subscriber Date of Birth:
YOUR INSURANCE INFORMATION
Relationship
to Subscriber?

YOUR INSURANCE INFORMATION
Is the relationship to subscriber correct?
Relationship to Subscriber:
YOUR INSURANCE INFORMATION
Group Name?

YOUR INSURANCE INFORMATION
Is the group name correct?
Name of Insurance:
YOUR SECONDARY INSURANCE INFORMATION
Do you have Secondary Insurance?

YOUR SECONDARY INSURANCE INFORMATION
Name of Secondary Insurance?
YOUR SECONDARY INSURANCE INFORMATION
Is the secondary insurance name correct?
Name of Insurance:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Claim's Address?

YOUR SECONDARY INSURANCE INFORMATION
Is the address correct?
Insurance Address:
,
YOUR SECONDARY INSURANCE INFORMATION
Secondary Phone Number?

YOUR SECONDARY INSURANCE INFORMATION
Is the phone number correct?
Insurance Phone Number:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Fax Number?

YOUR SECONDARY INSURANCE INFORMATION
Is the fax correct?
Insurance Fax Number:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Subscriber ID?

YOUR SECONDARY INSURANCE INFORMATION
Is the subscriber ID correct?
Subscriber ID:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Subscriber Name?

YOUR SECONDARY INSURANCE INFORMATION
Is the subscriber's name correct?
Subscriber Name:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Subscriber's Date of Birth?

YOUR SECONDARY INSURANCE INFORMATION
Is the subscriber's date of birth correct?
Subscriber Date of Birth:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Relationship to Subscriber?

YOUR SECONDARY INSURANCE INFORMATION
Is the relationship to subscriber correct?
Relationship to Subscriber:
YOUR SECONDARY INSURANCE INFORMATION
Secondary Group Name?

YOUR SECONDARY INSURANCE INFORMATION
Is the group name correct?
Group Name:
SECONDARY INFORMATION
Medicare Number?
SECONDARY INFORMATION
Is the Medicare number correct?
Medicare Number:
SECONDARY INFORMATION
Medicare State?

SECONDARY INFORMATION
Is the Medicare state correct?
Medicare State:
MEDICARE INFORMATION
Medicare Number?
MEDICARE INFORMATION
Is the Medicare number correct?
Medicare Number:
MEDICARE INFORMATION
Medicare State?
MEDICARE INFORMATION
Is the Medicare state correct?
Medicare State:
MEDICARE INFORMATION
Medicare Subscriber Name?
Subscriber Name:
RELEASE & AUTHORIZATION
I, , authorize the release of any medical or other information necessary to determine eligibility and if I decide to proceed with the sleep appliance, seek reimbursement for the sleep appliance. I am giving American Sleep Dentistry the authorization and their affiliates to use information that may be confidential, privileged, and protected by law.
After American Sleep Dentistry provides me with any out-of-pocket expense, if I decide to proceed with the sleep appliance, I authorize payments for the sleep appliance furnished to me by American Sleep Dentistry to be paid directly to American Sleep Dentistry. I authorize payments for the sleep test furnished to me by iSleep Physician Group PC to be paid directly to iSleep Physician Group PC. I agree that I am responsible for payment of the cost of services that my insurance company does not pay, as well as any copayment or deductible for which I am responsible.
I appoint American Sleep Dentistry and iSleep Physician Group PC to act as my representative in connection with my claim or asserted right under Title 18 of the Social Security Act (the Act) and related provisions of Title 11 of the Act. I authorize this individual to make any request; to present or to elicit evidence; to obtain appeals information; and to receive any notice in connection with my claim, appeal, grievance or request wholly in my stead. I understand that personal medical information related to my appeal may be disclosed to the representative indicated below.
Callback
I'll call you back in 30 minutes at
INTEREST LEVEL
On a scale of 1-10 how likely are you to move forward?

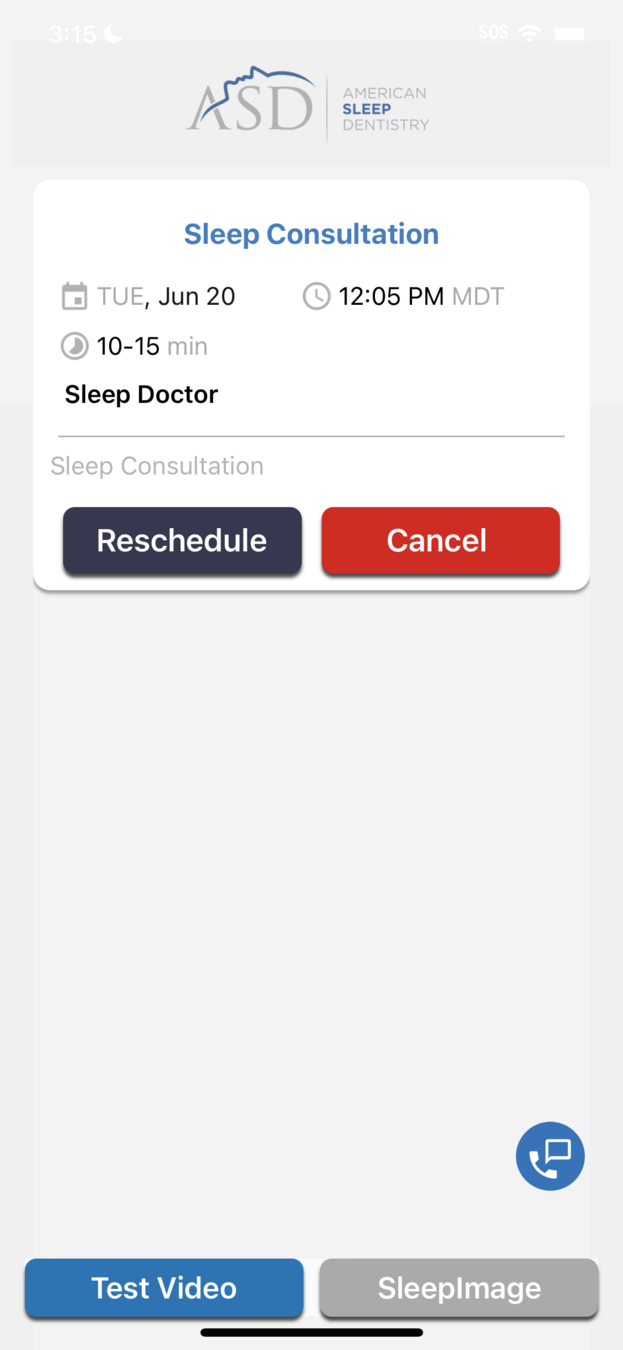
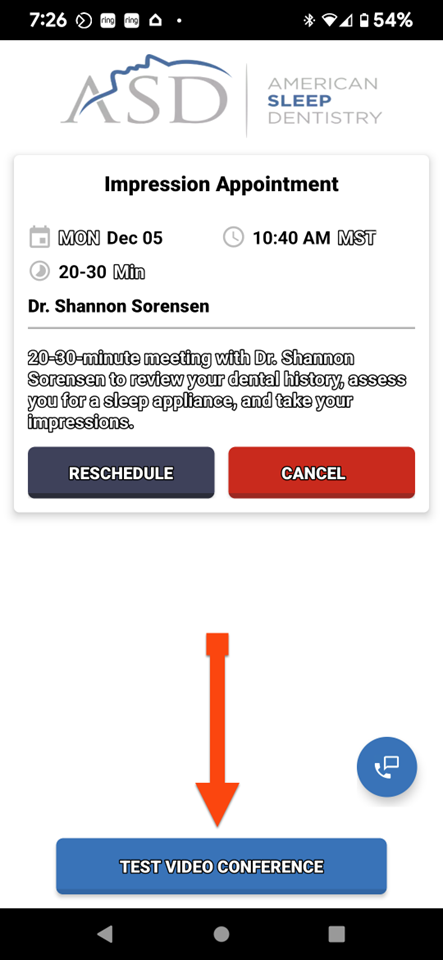
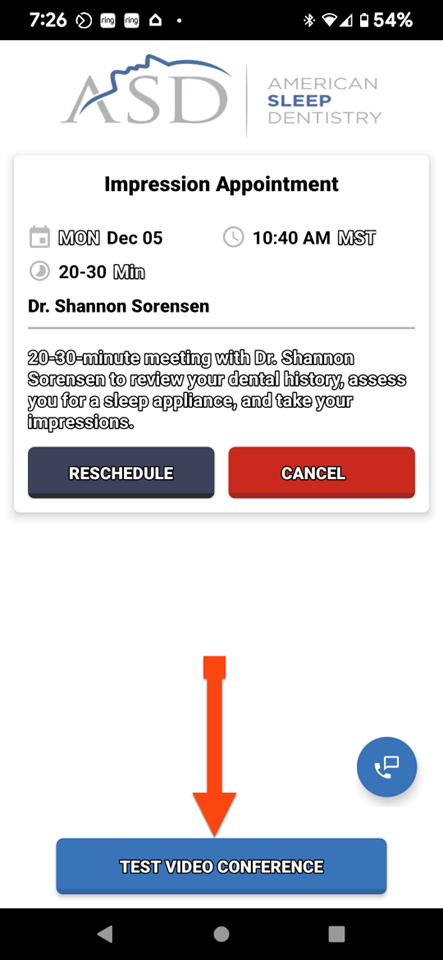
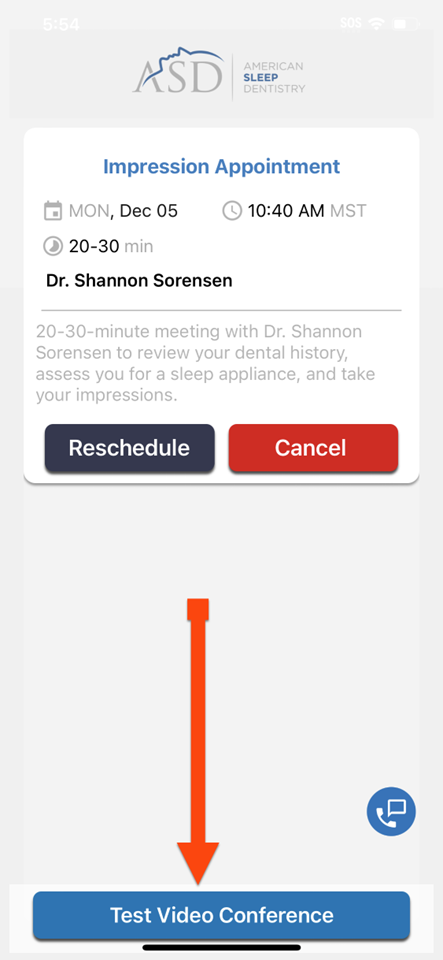
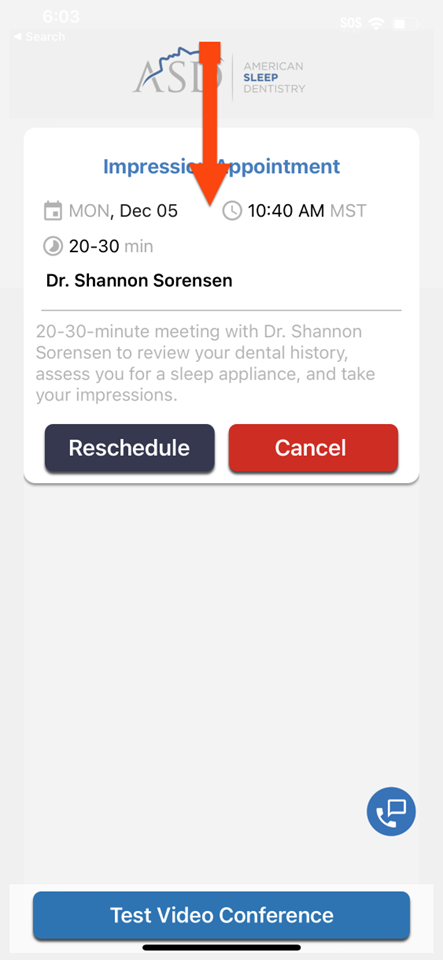
APPOINTMENT DATE & TIME

APPOINTMENT DATE & TIME
Date:
Time:
APPOINTMENT DATE & TIME
Date:
Time:
YOUR INSURANCE INFORMATION
MEDICARE BENEFITS
Out of Pocket Expenses
Deductible
Coinsurance
Secondary Insurance
Out-of-Pocket Expense
___________________________
MEDICARE BENEFITS
Out of Pocket Expenses
Payment Plan
payments of
Payment due after fitting of sleep appliance
MEDICARE BENEFITS
Deductible Remaining After Receiving OA
MEDICARE BENEFITS
1 Payment
Payment Plan
payments of
Payment due after fitting of sleep appliance
MEDICARE BENEFITS
How many persons reside in your household?
How many people are in your family?
How much money did you report on your taxes last year?
MEDICARE BENEFITS
How much can you afford each month?
MEDICARE BENEFITS
Pay $0 until after you are fitted with a sleep appliance

Sleep Test
Charged $0 if you return sleep test.
Charged $200 if you do not return sleep test.
PAYMENT INFORMATION
Name on Credit Card?

PAYMENT INFORMATION
Billing Address?

PAYMENT INFORMATION
Address:
,
Is your billing information correct?
PAYMENT INFORMATION
Credit Card Number?

PAYMENT INFORMATION
Credit Card
Expiration Date?

PAYMENT INFORMATION
Credit Card
Security Code?

PAYMENT INFORMATION
Credit Card Number:
Expiration Date:
Security Number:
Is your credit card information correct?
PAYMENT FORM
INSURANCE BENEFITS
Out of Pocket Expenses
Deductible
Coinsurance
Secondary Insurance
Out-of-Pocket Expense
___________________________
INSURANCE BENEFITS
Out of Pocket Expenses
Payment Plan
payments of
Payment due after fitting of sleep appliance
INSURANCE BENEFITS
Deductible Remaining After Receiving OA
INSURANCE BENEFITS
1 Payment
Payment Plan
payments of
Payment due after fitting of sleep appliance
INSURANCE BENEFITS
How many persons reside in your household?
How many people are in your family?
How much money did you report on your taxes last year?
INSURANCE BENEFITS
We will waive your coinsurance.
$50 month payment.
INSURANCE BENEFITS
How much can you afford each month?
INSURANCE BENEFITS
Pay $0 until after you are fitted with a sleep appliance
Sleep Test
Charged $0 if you return sleep test.
Charged $200 if you do not return sleep test.
PAYMENT INFORMATION
Name on Credit Card?
PAYMENT INFORMATION
Billing Address?
PAYMENT INFORMATION
Address:
,
Is your billing information correct?
PAYMENT INFORMATION
Credit Card Number?
PAYMENT INFORMATION
Credit Card
Expiration Date?
PAYMENT INFORMATION
Credit Card
Security Code?
PAYMENT INFORMATION
Credit Card Number:
Expiration Date:
Security Number:
Is your credit card information correct?
INSURANCE BENEFITS
Out of Pocket Expenses
Deductible
Coinsurance
Secondary Insurance
Out-of-Pocket Expense
___________________________
INSURANCE BENEFITS
Out of Pocket Expenses
Payment Plan
payments of
Payment due after fitting of sleep appliance
INSURANCE BENEFITS
Deductible Remaining After Receiving OA
INSURANCE BENEFITS
1 Payment
Payment Plan
payments of
Payment due after fitting of sleep appliance
INSURANCE BENEFITS
How many persons reside in your household?
How many people are in your family?
How much money did you report on your taxes last year?
INSURANCE BENEFITS
We will waive your coinsurance.
$50 month payment.
INSURANCE BENEFITS
How much can you afford each month?
INSURANCE BENEFITS
Pay $0 until after you are fitted with a sleep appliance
Sleep Test
Charged $0 if you return sleep test.
Charged $200 if you do not return sleep test.
PAYMENT INFORMATION
Name on Credit Card?
PAYMENT INFORMATION
Billing Address?
PAYMENT INFORMATION
Address:
,
Is your billing information correct?
PAYMENT INFORMATION
Credit Card Number?
PAYMENT INFORMATION
Credit Card
Expiration Date?
PAYMENT INFORMATION
Credit Card
Security Code?
PAYMENT INFORMATION
Is your credit card information correct?
Credit Card Number:
Expiration Date:
Security Number:
INTEREST LEVEL
On a scale of 1-10 how likely are you to move forward?
INTEREST FREE PAYMENT PLAN
Interest: 0%
Payments: $50
Number of Payments: 18
INTEREST LEVEL
On a scale of 1-10 how likely are you to move forward?
PAYMENT INFORMATION
Name on Credit Card?
PAYMENT INFORMATION
Billing Address?
PAYMENT INFORMATION
Address:
,
Is your billing information correct?
PAYMENT INFORMATION
Credit Card Number?
PAYMENT INFORMATION
Credit Card
Expiration Date?
PAYMENT INFORMATION
Credit Card
Security Code?
PAYMENT INFORMATION
Credit Card Number:
Expiration Date:
Security Number:
Is your credit card information correct?
CONSENT
I, , authorize that payments for medical supplies furnished to me by American Sleep Dentistry, be paid directly to American Sleep Dentistry. I agree to 18 interest-free monthly payments of $50 each for a total of $900.
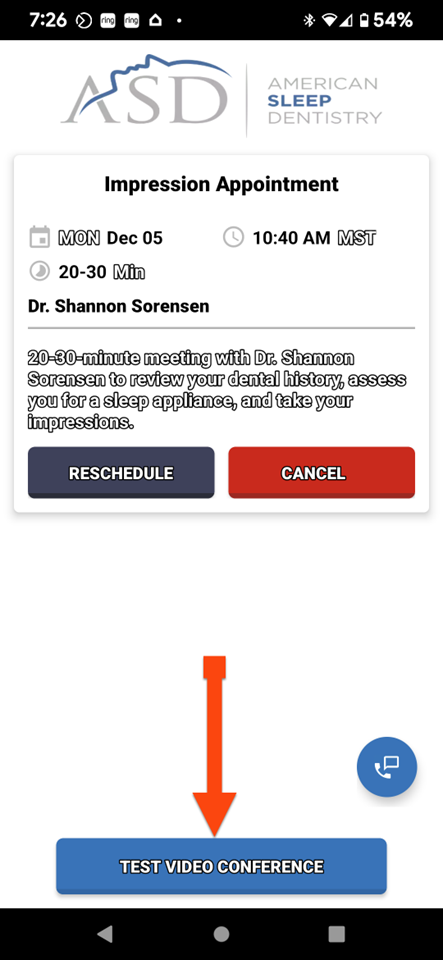
SCHEDULE TELEHEALTH APPOINTMENT
What time zone?
TIME ZONE
Is your time zone correct?
Your Time Zone:
APPOINTMENT DATE & TIME
APPOINTMENT DATE & TIME
Date:
Time:
I consent to engaging in Telehealth with ASD Sleep and iSleep Physician Group PC. I understand that “telemedicine or Telehealth” includes the practice of health care delivery, diagnosis, consultation, treatment, transfer of medical data, and education using interactive audio, video, or data communications. I understand that Telehealth also involves the communication of my medical, both orally and visually, to health care practitioners.
I understand that I have the following rights with respect to Telehealth:
- I have the right to withhold or withdraw consent at any time without affecting my right to future care or treatment or risking the loss or withdrawal of any benefits to which I would otherwise be entitled.
- The laws that protect the confidentiality of my medical information also apply to Telehealth. As such, I understand that the information disclosed by me during my Telehealth visit is generally confidential.
- I understand that there are risks and consequences from Telehealth, including, but not limited to, the possibility that: the transmission of my medical information could be disrupted or distorted by technical failures; the transmission of my medical information could be interrupted by unauthorized persons; and/or the electronic storage of my medical information could be accessed by unauthorized persons.
- I understand that I may benefit from telemedicine, but that results cannot be guaranteed or assured.
- I understand that I have a right to access my medical information and copies of medical records in accordance with the law.
- In addition, I understand that if the dentist believes I would be better served by face-to-face services, I will be referred to another healthcare provider who can provide such services in my area.
- If you have an emergency, please Call 911. If it is not an emergency, you can call 800.555.1518.
- You agree that your credit card will be charged $0 if the sleep test is returned. In the event that the sleep test is not returned, you consent that your credit card can be charged $200.
- My medical insurance or Medicare will be billed for a sleep consultation, sleep test and diagnosis by a third party. My credit card maybe charged a maximum of $40 if my medical insurance or Medicare does not cover the cost of the sleep consultation and shipping, sleep test and diagnosis.
CONSENT TO TELEHEALTH
YOUR PERSONAL INFORMATION
Cell Number?
YOUR PERSONAL INFORMATION
Cell Number:
Is your cell number correct?
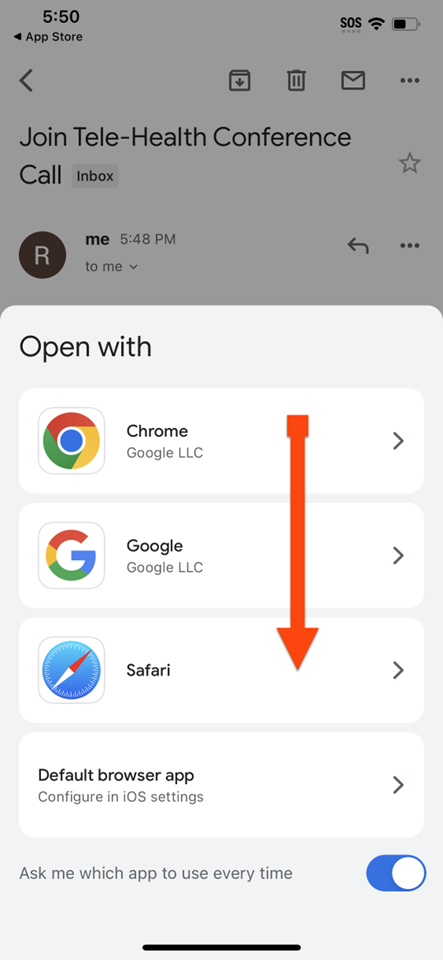
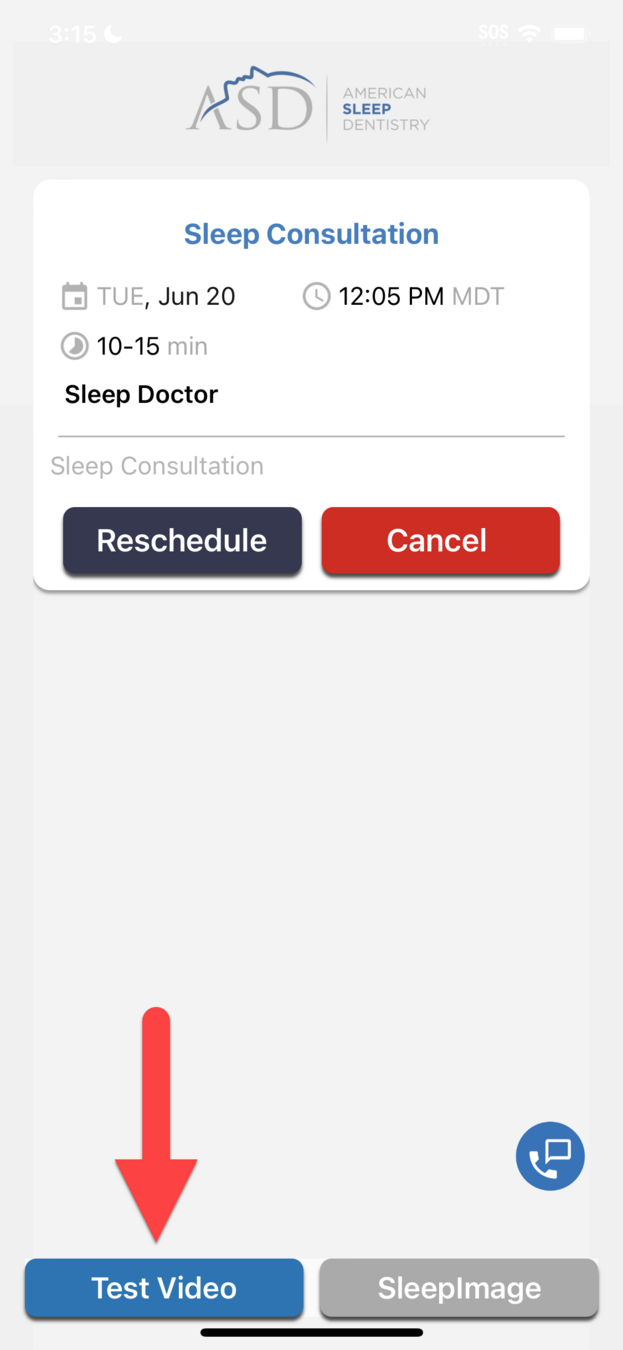
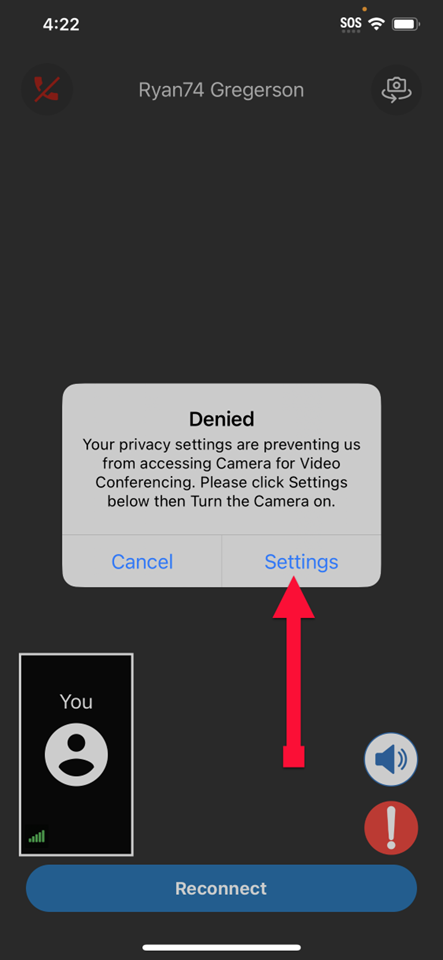
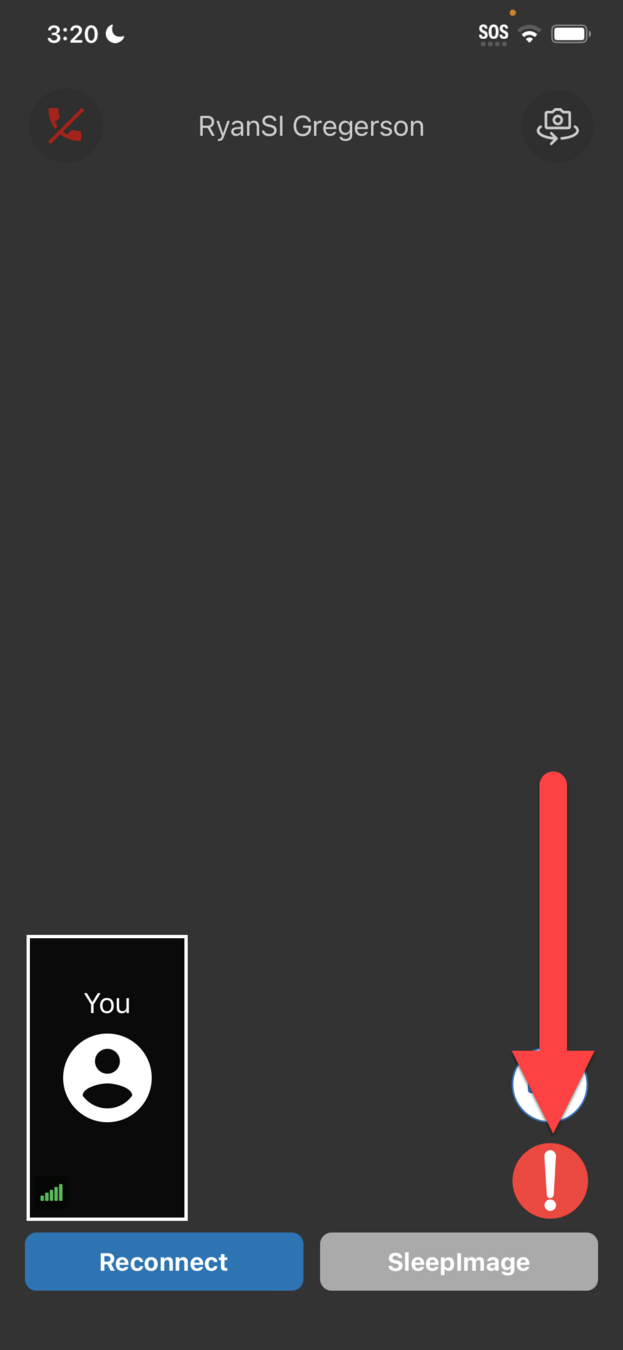
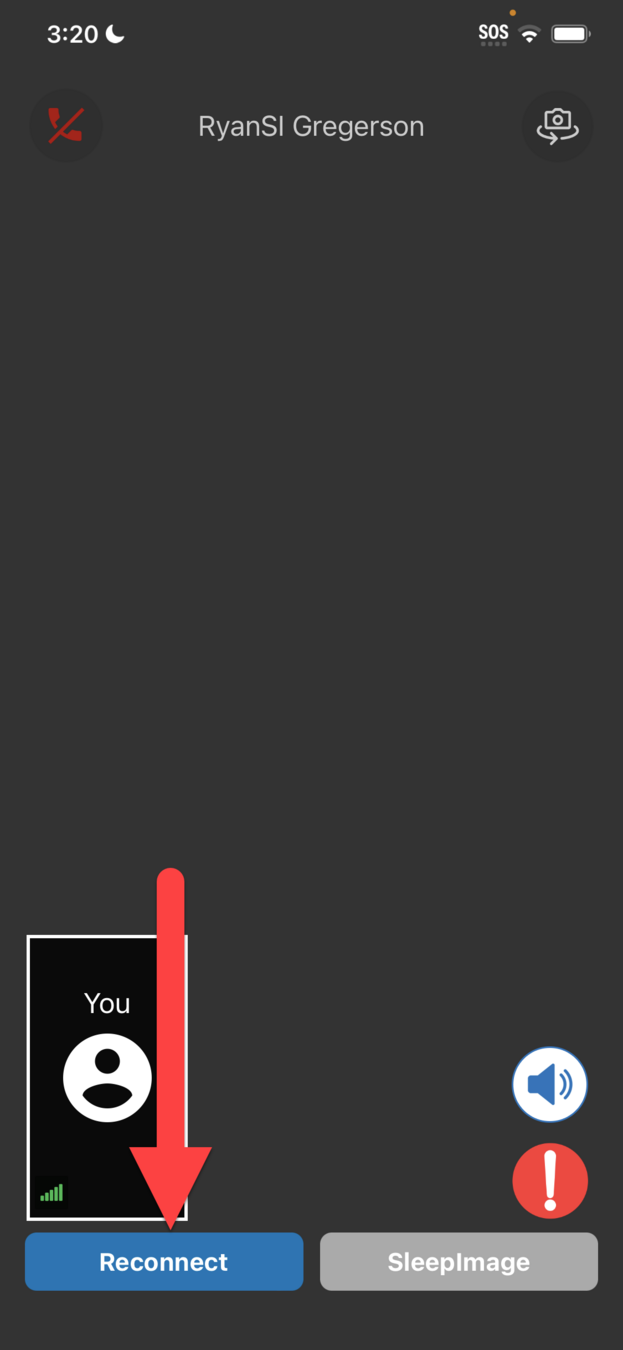
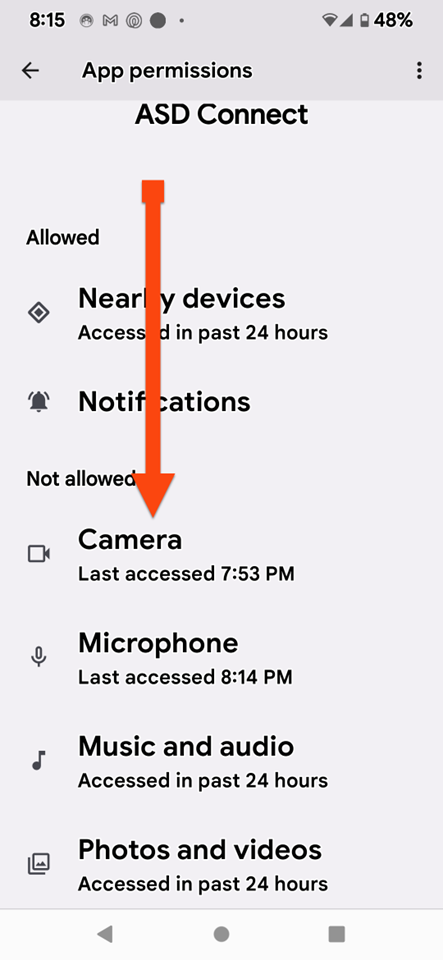
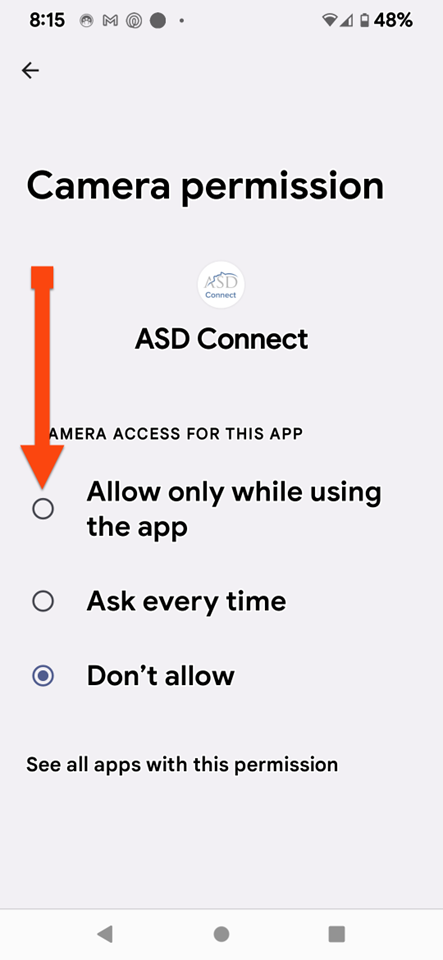
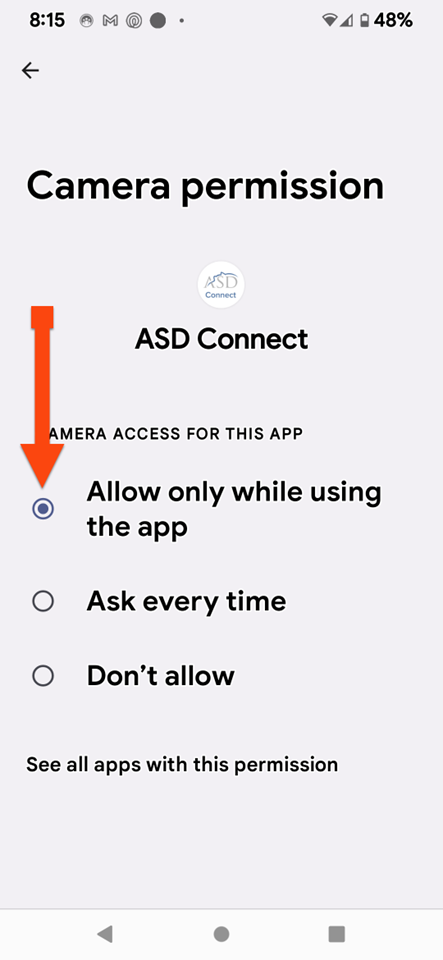
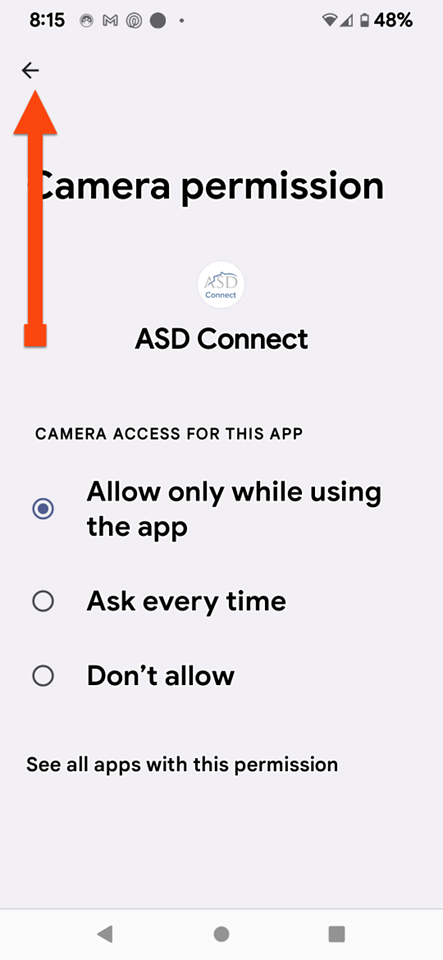
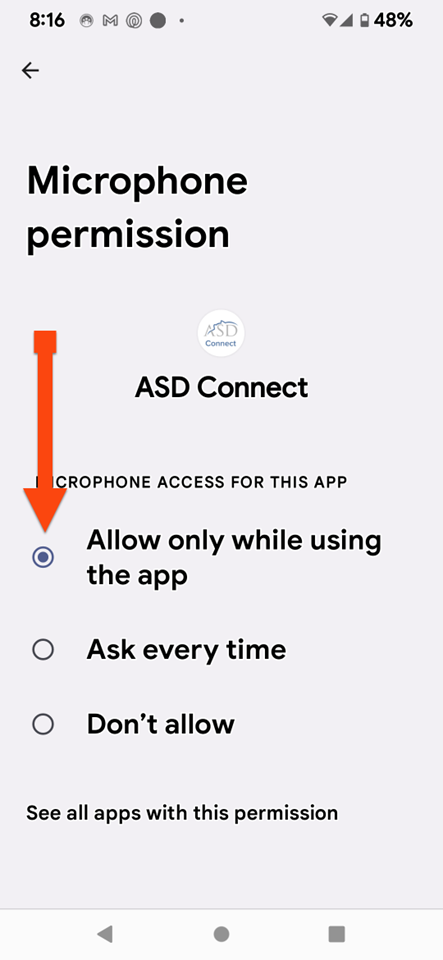
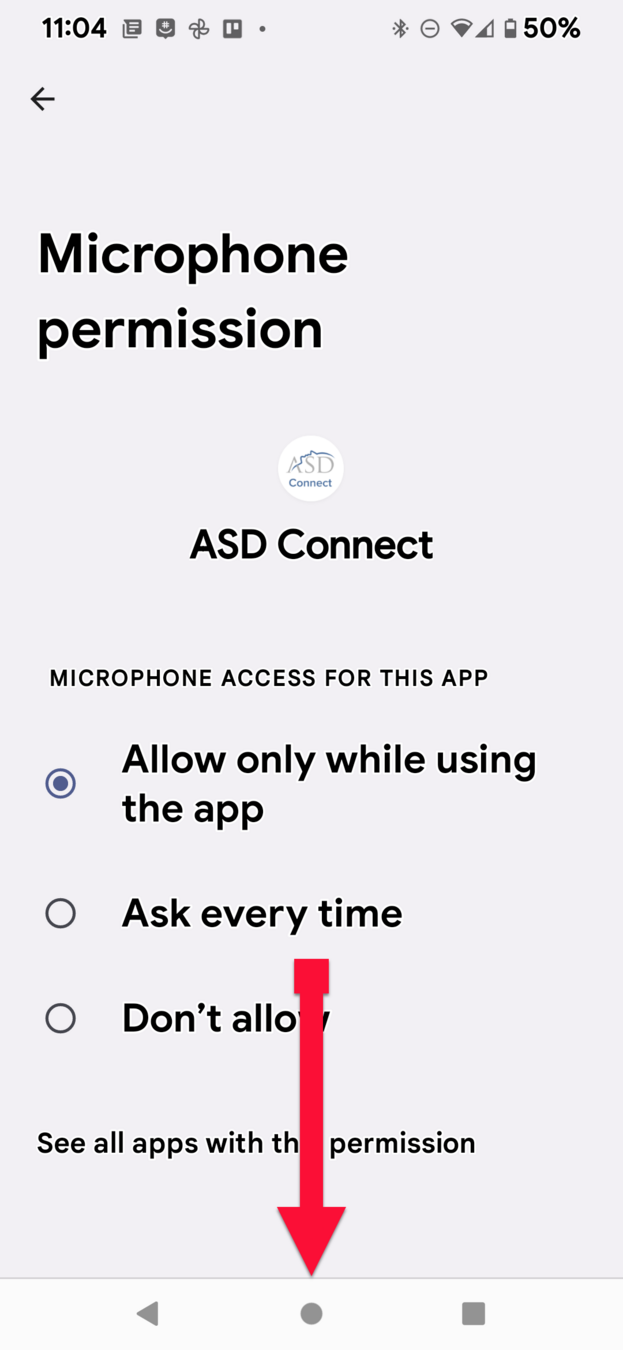
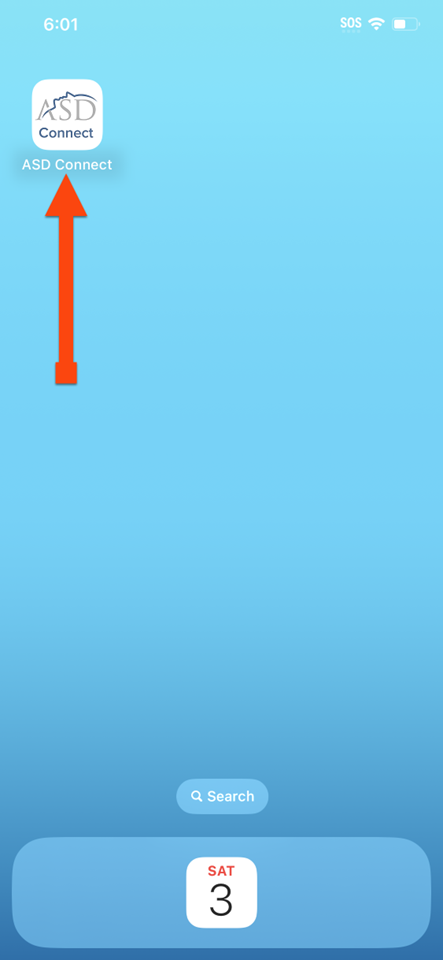
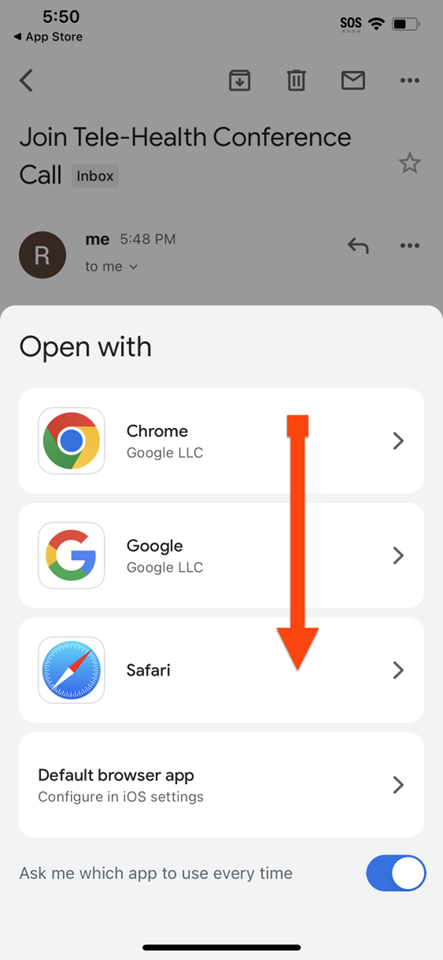
CLICK ON PHONE

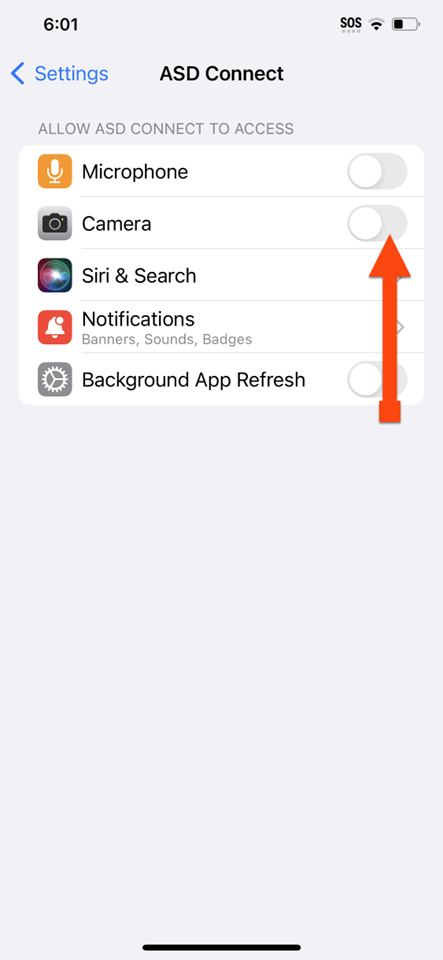
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
iPHONE
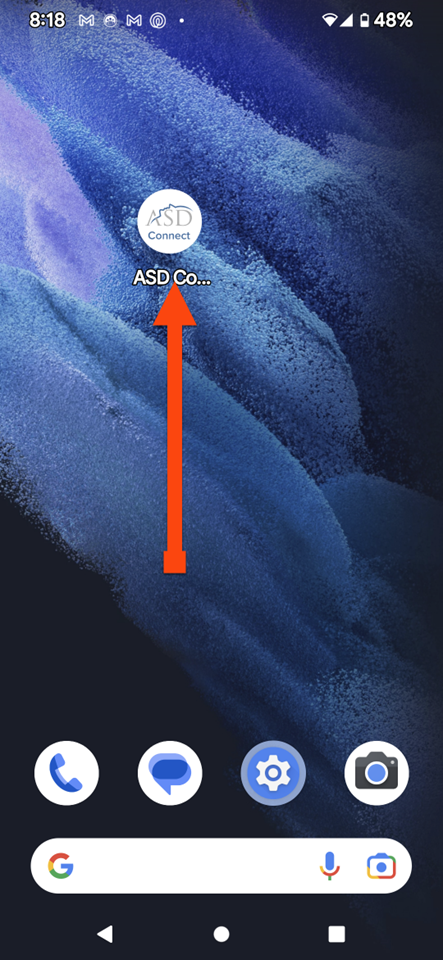
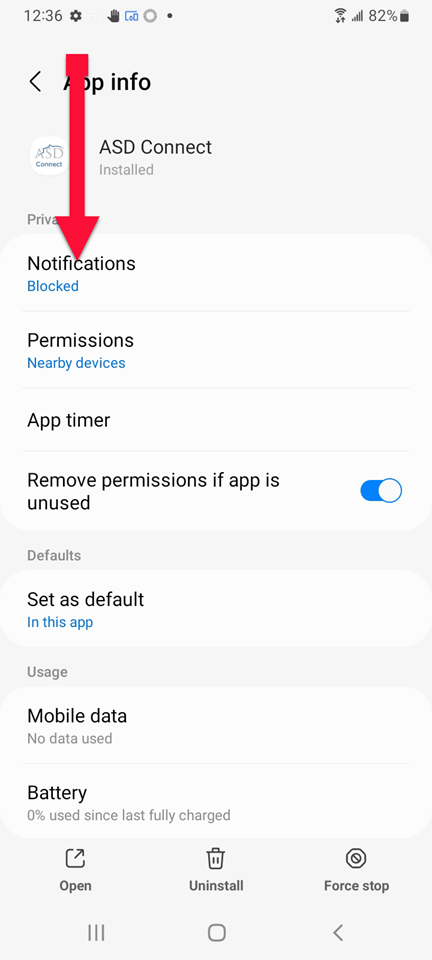
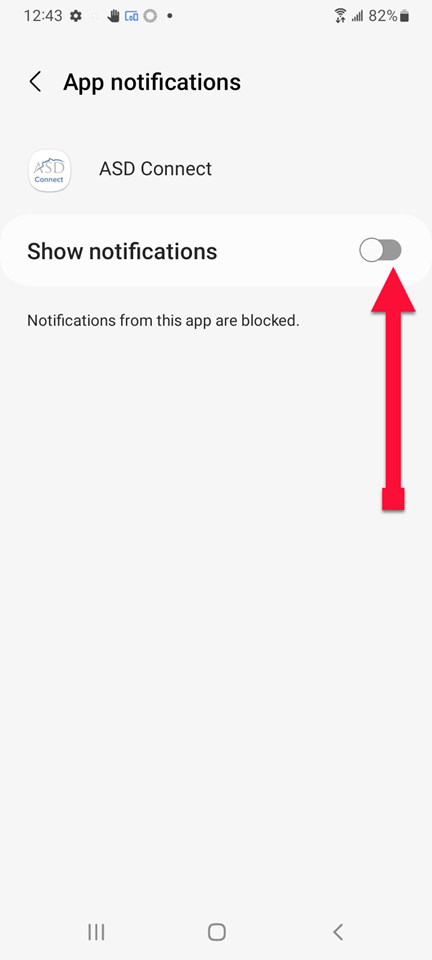
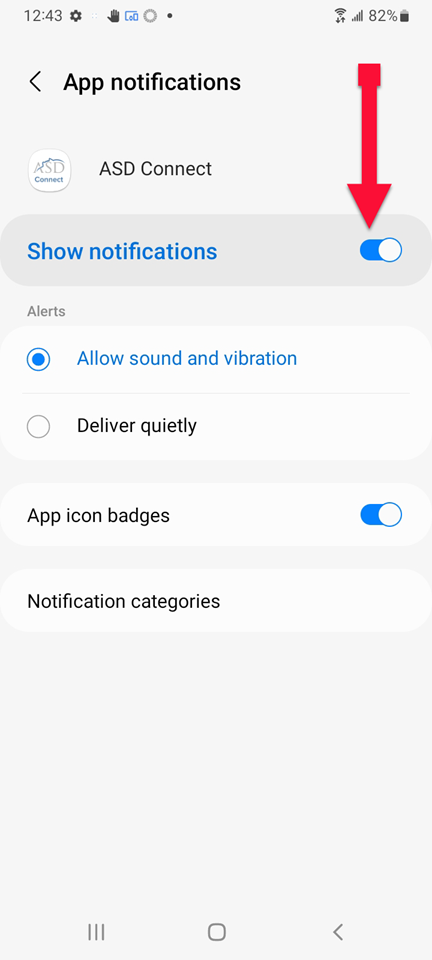
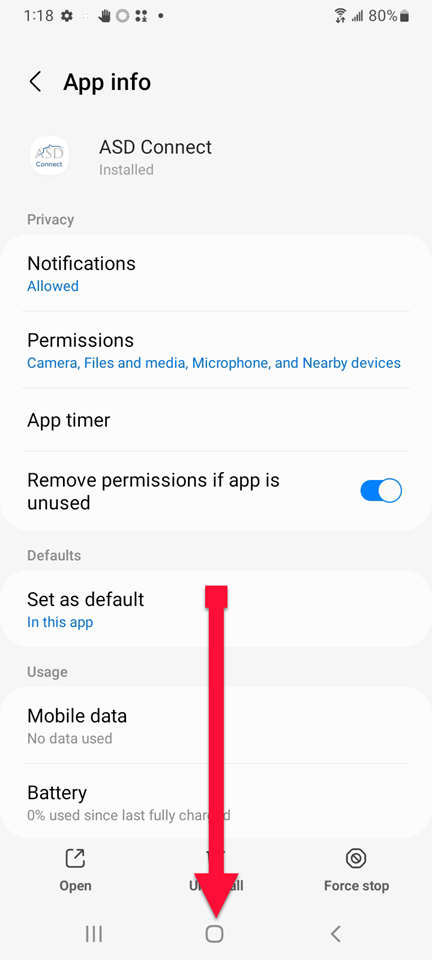
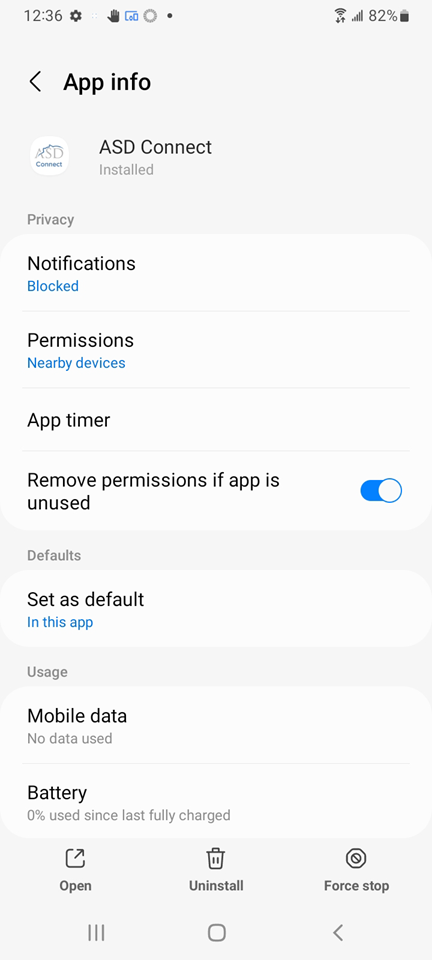
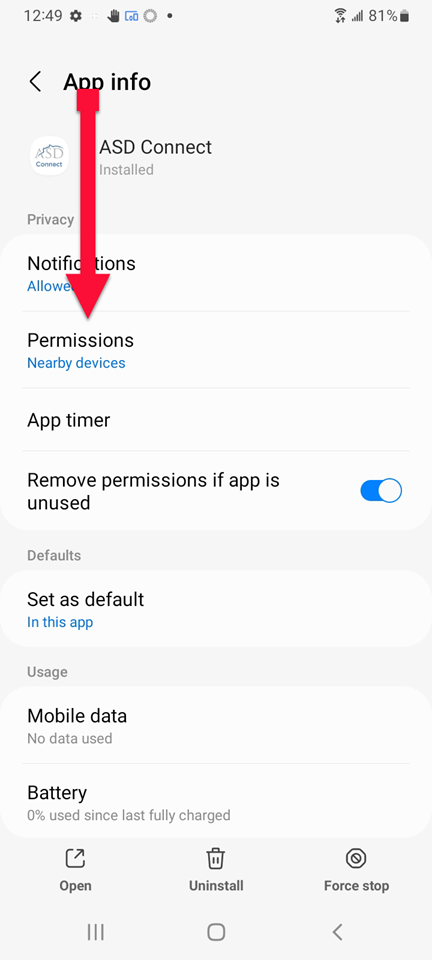
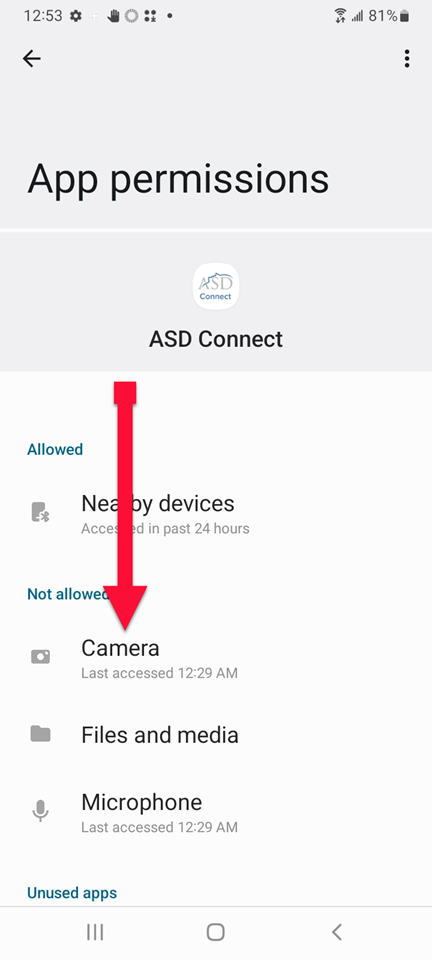
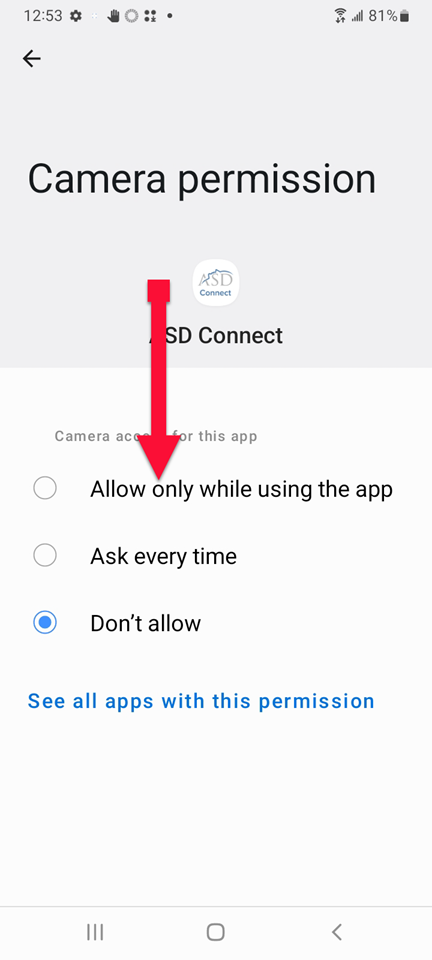
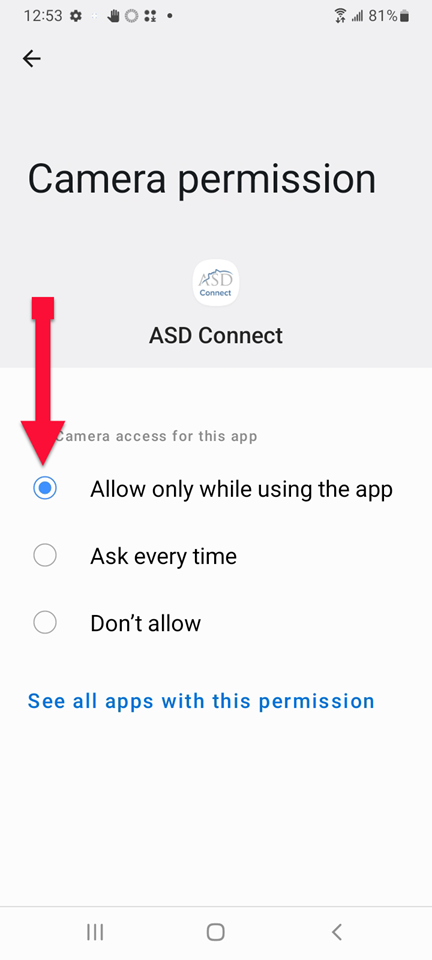
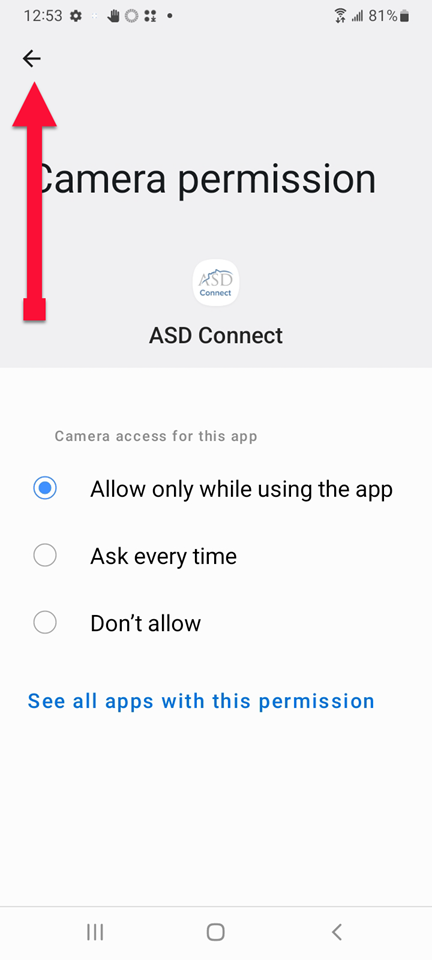
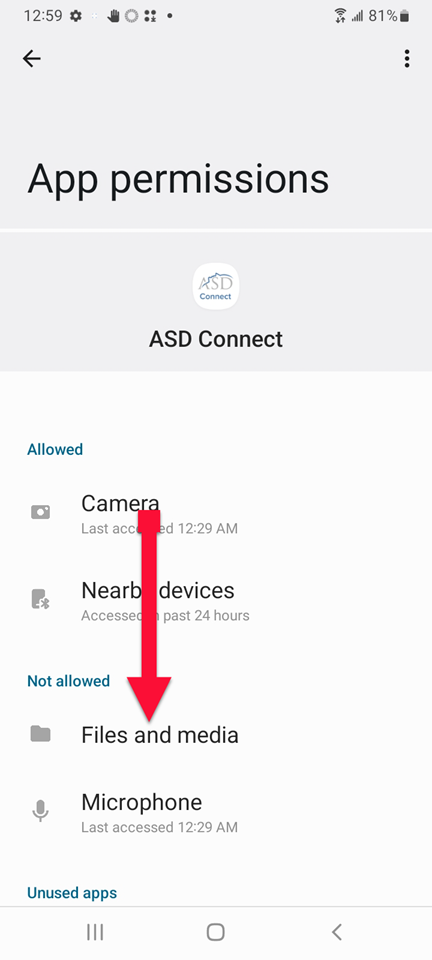
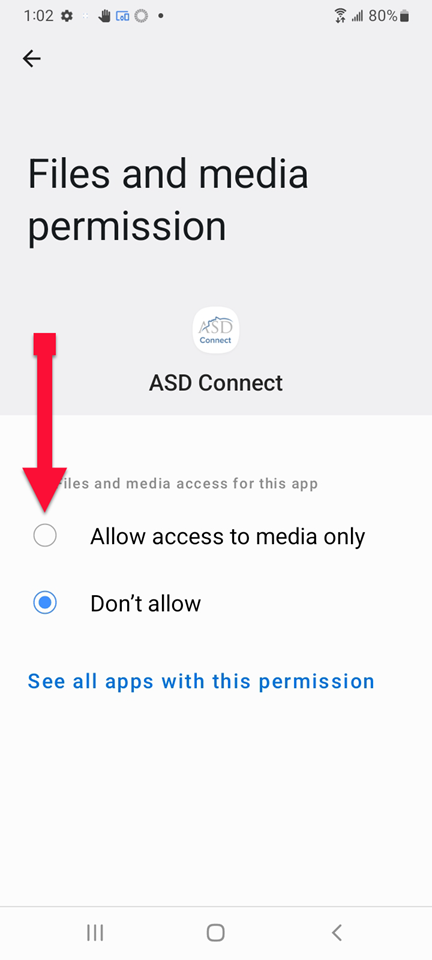
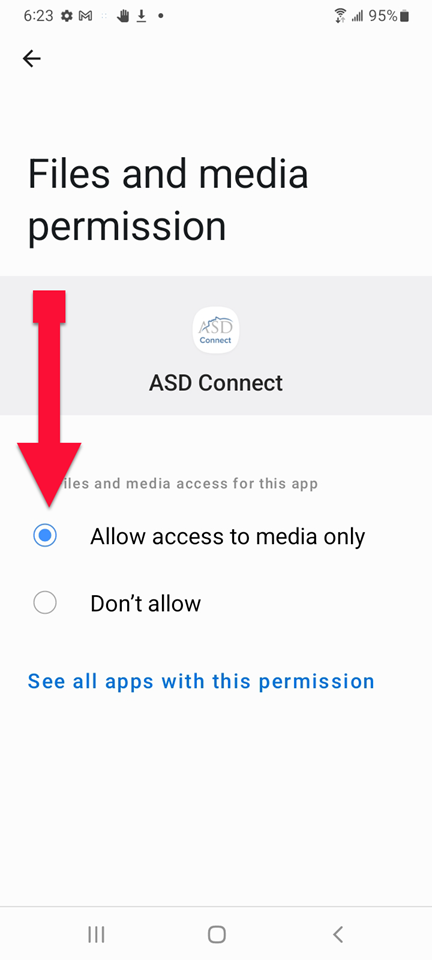
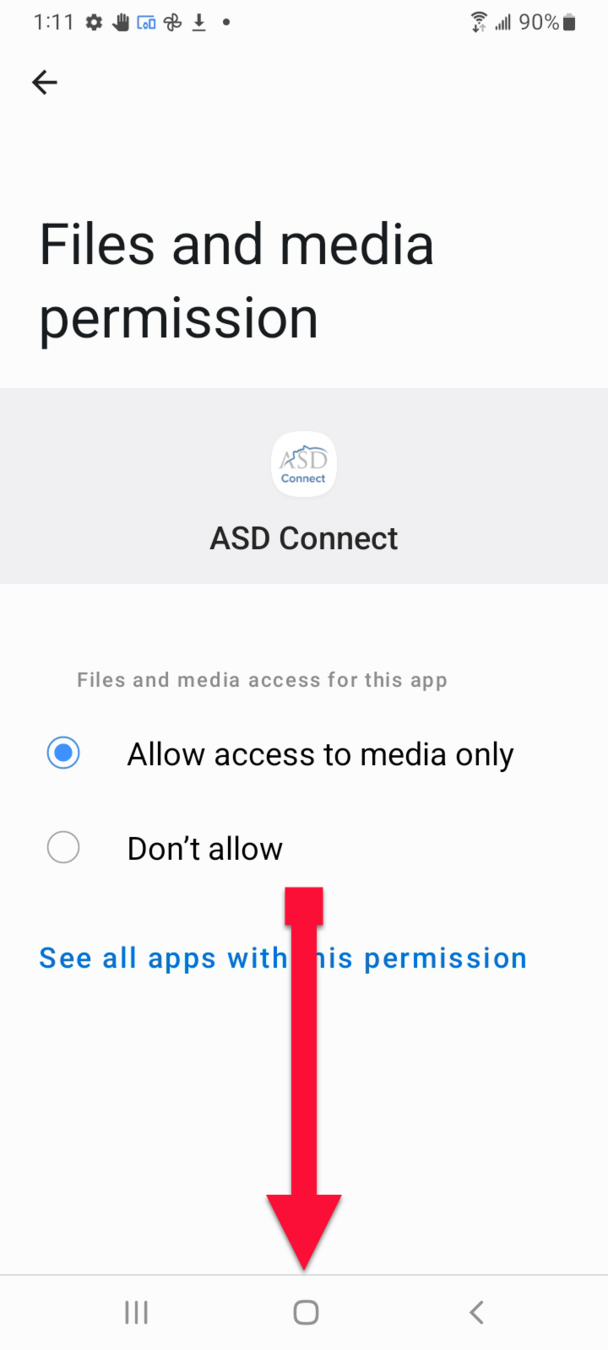
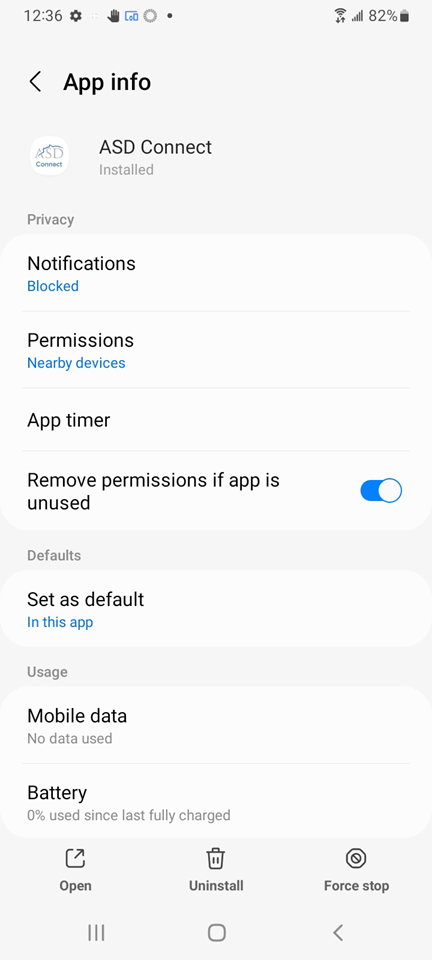
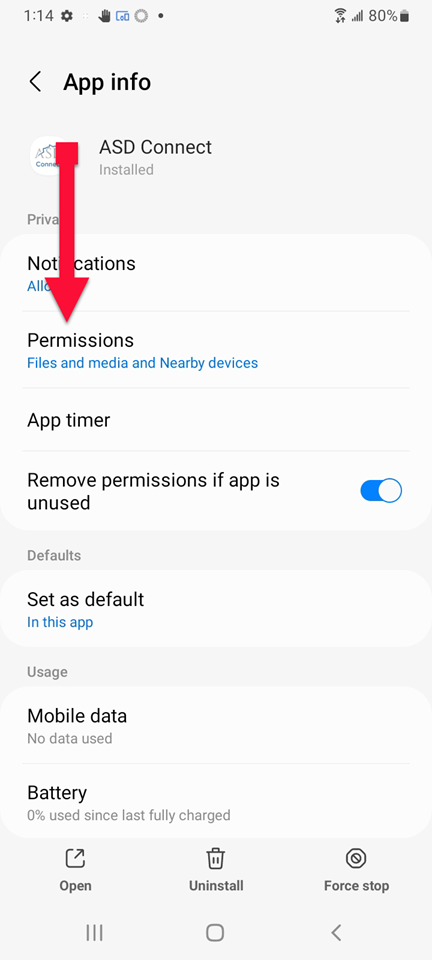
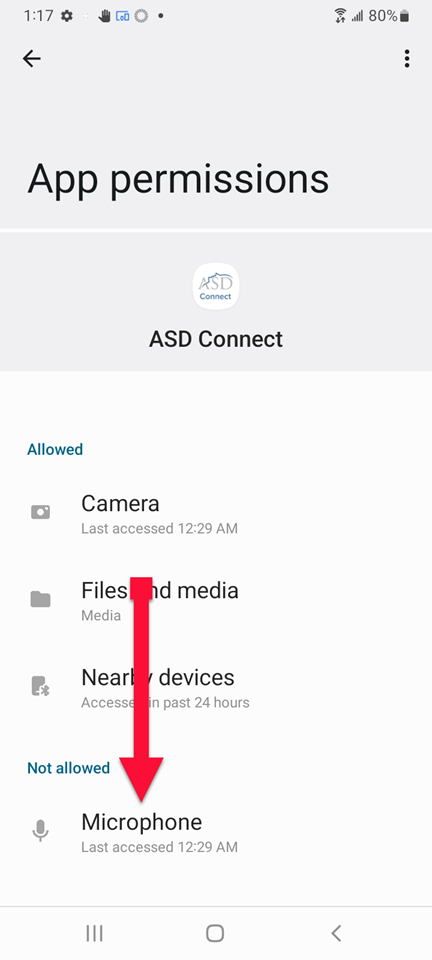
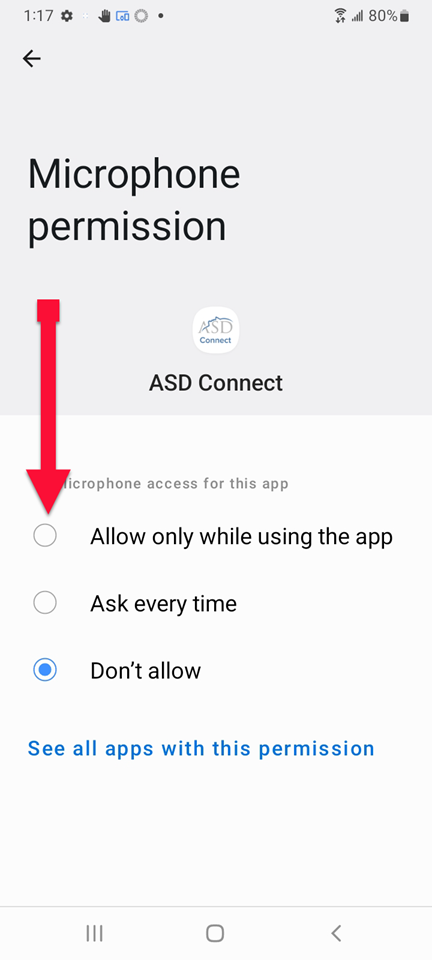
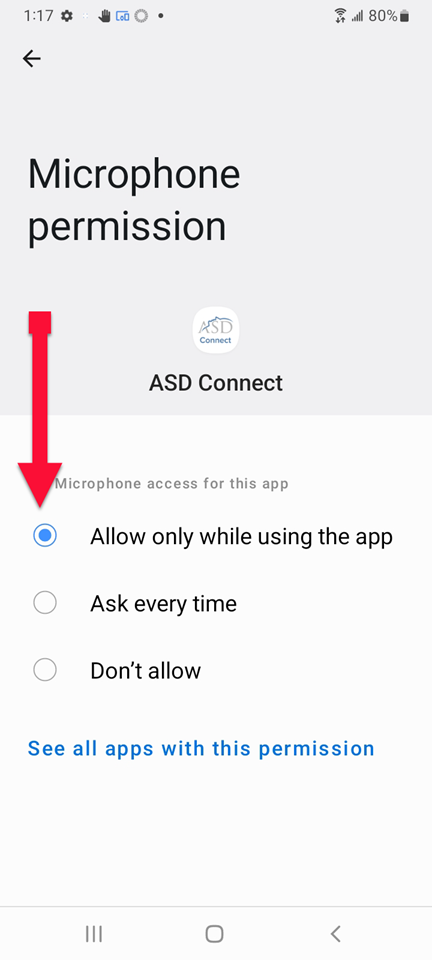
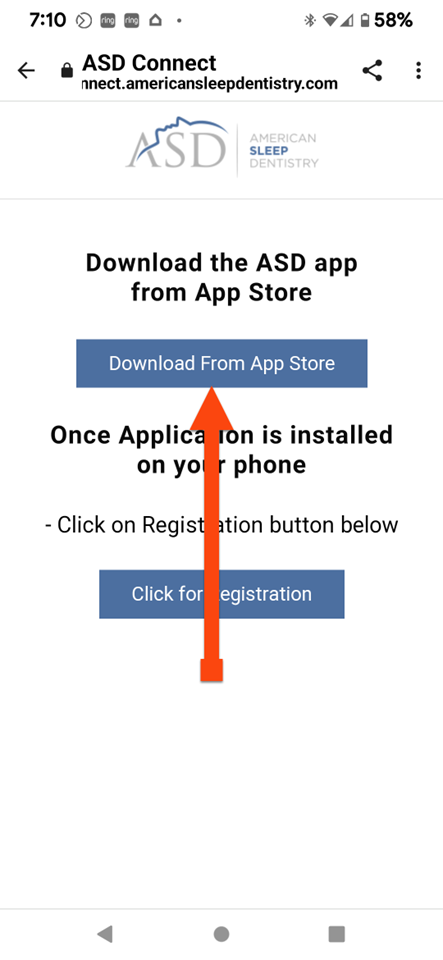
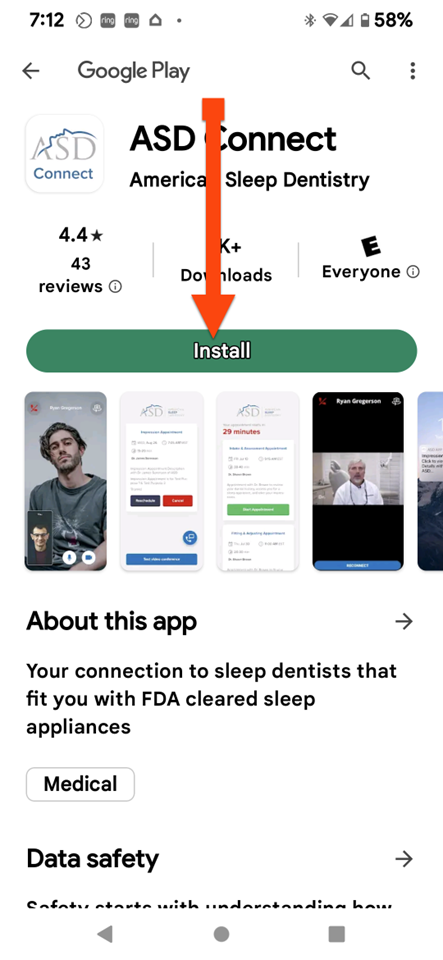
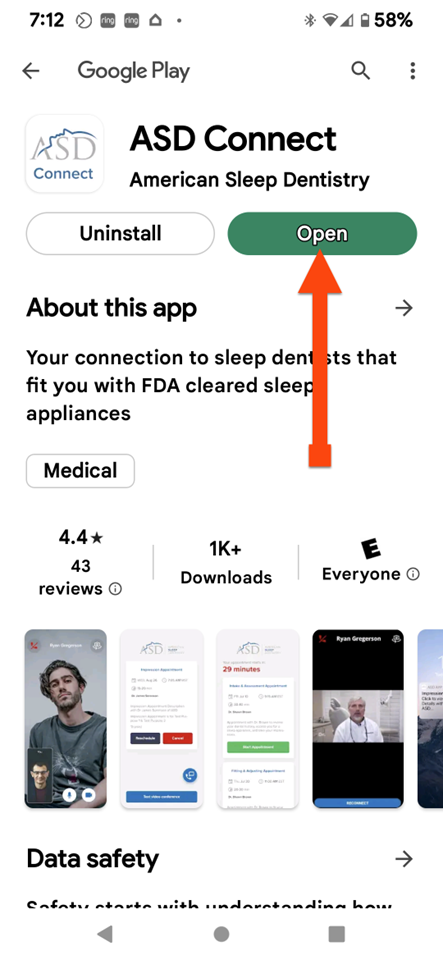
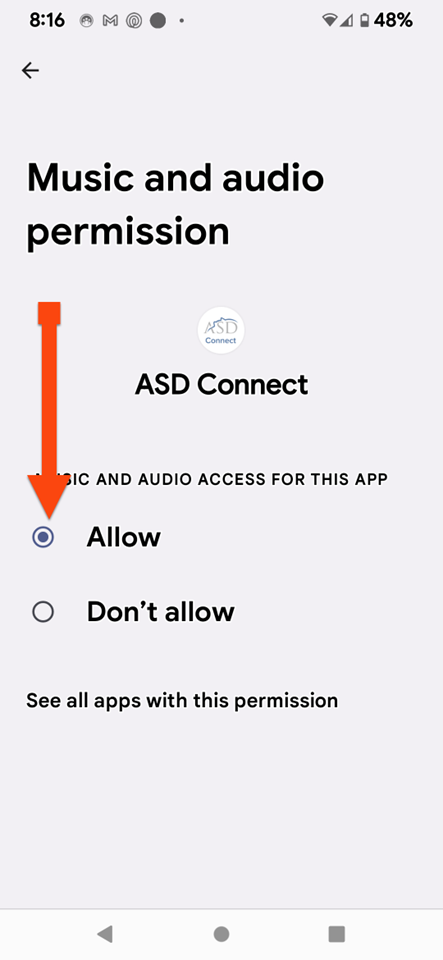
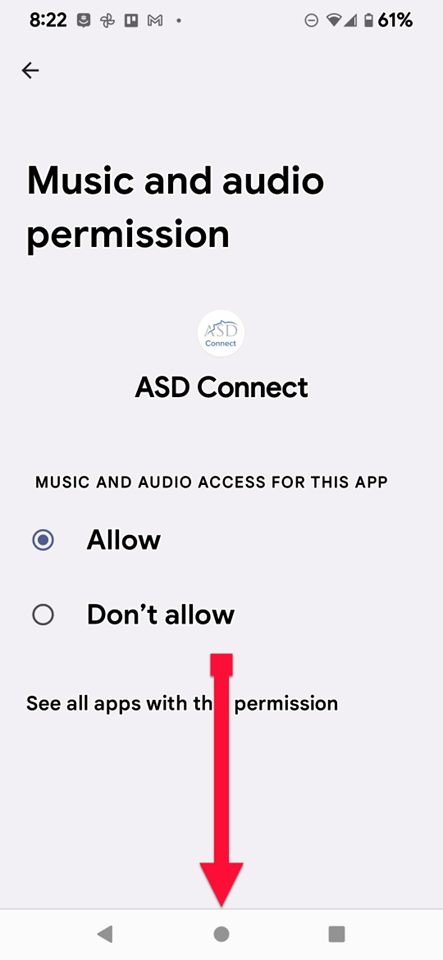
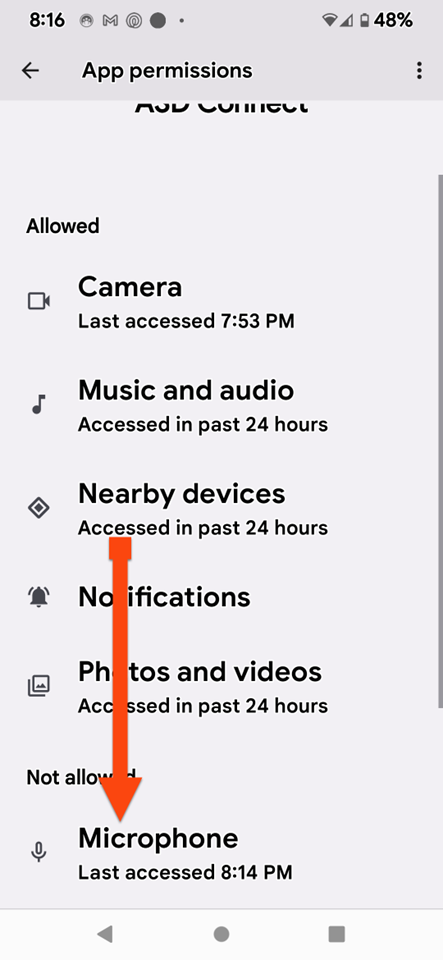
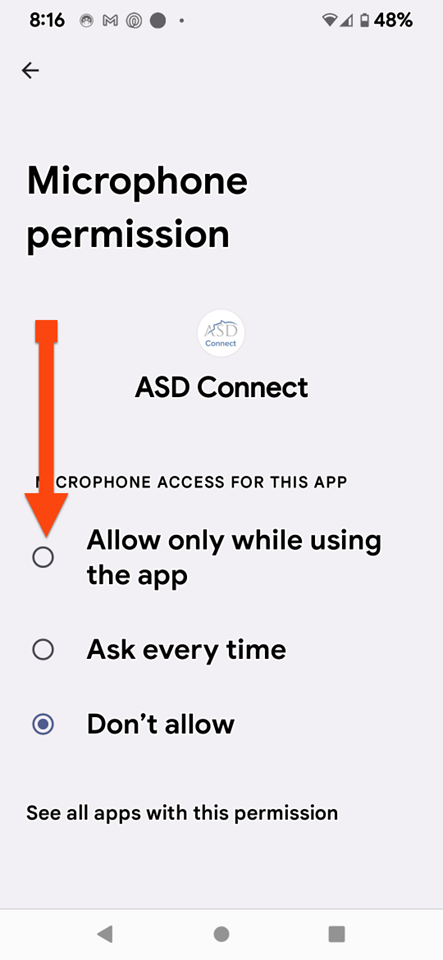
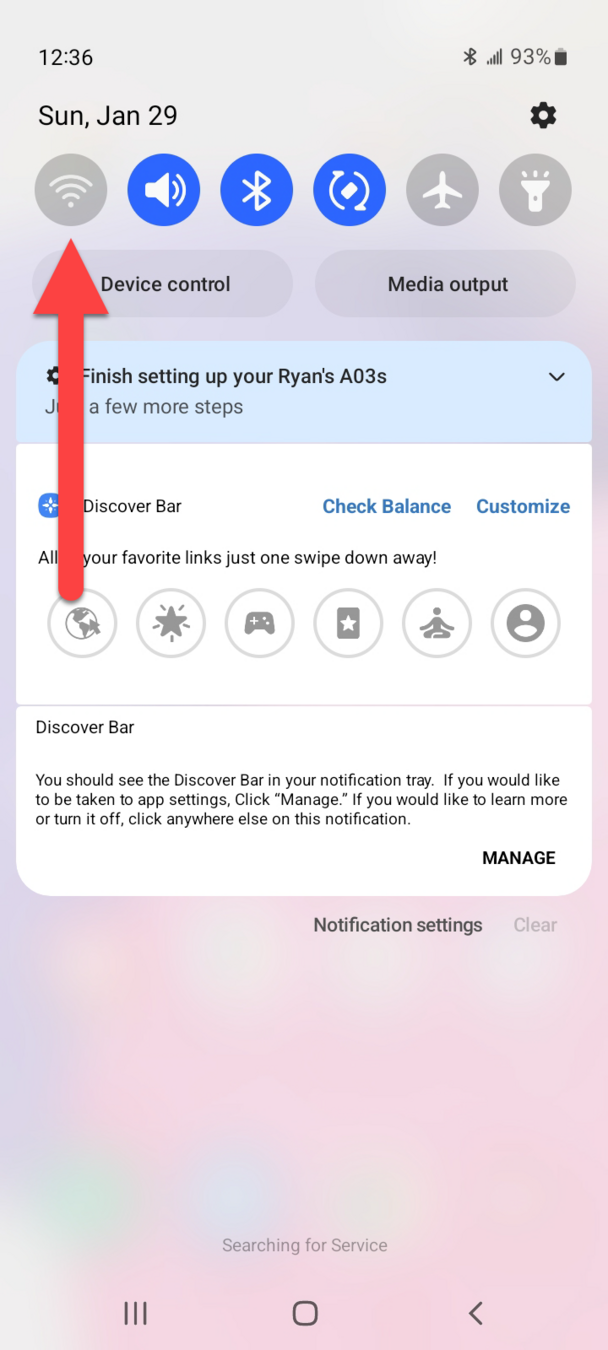
ANDROID
ANDROID

ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID

ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID

ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
ANDROID
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL
PIXEL

Dr.
The sleep specialist will be with you shortly.
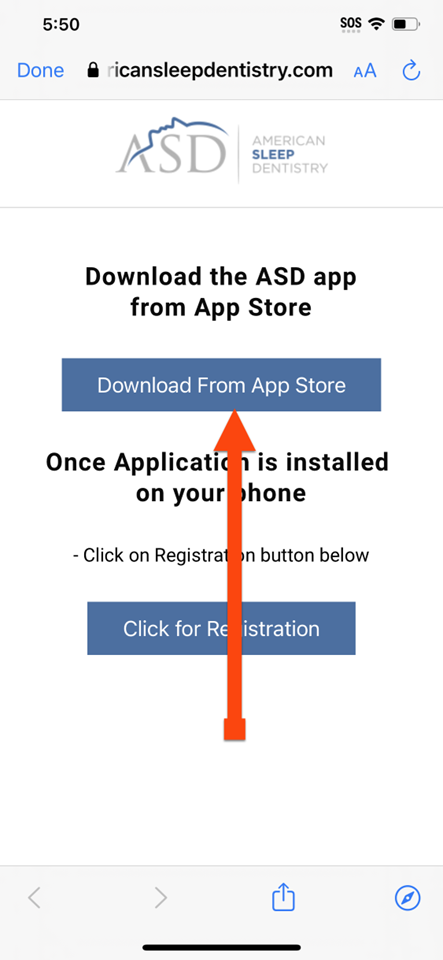
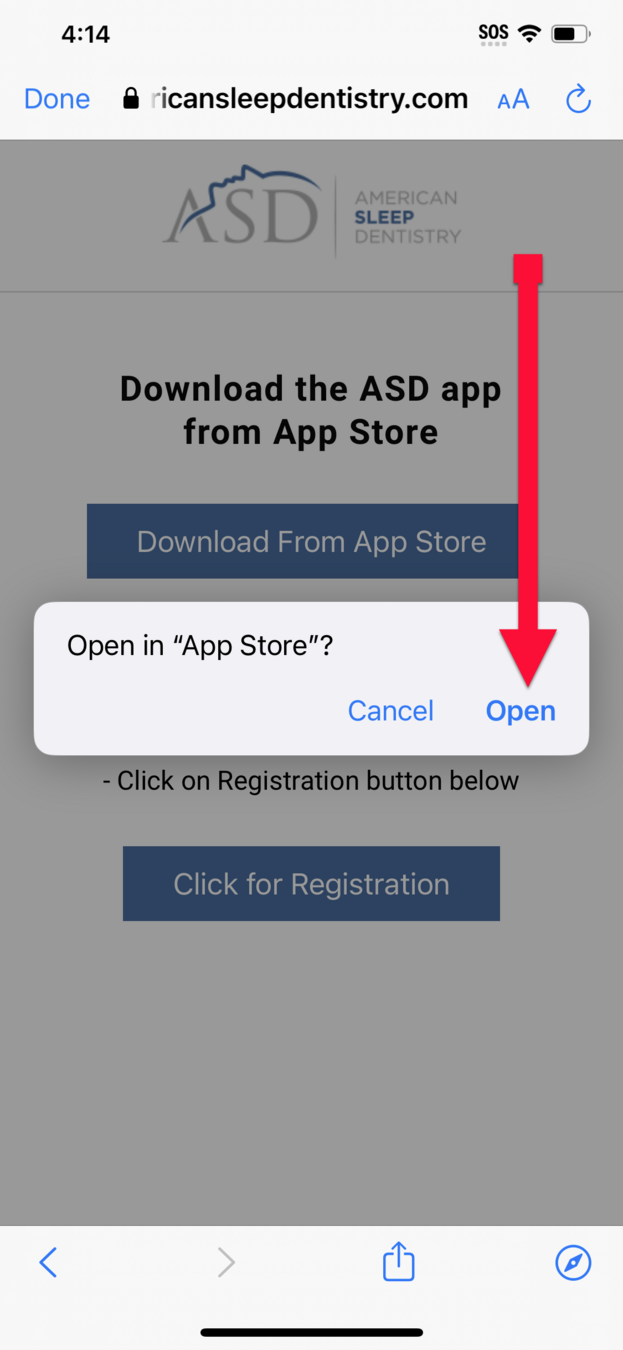
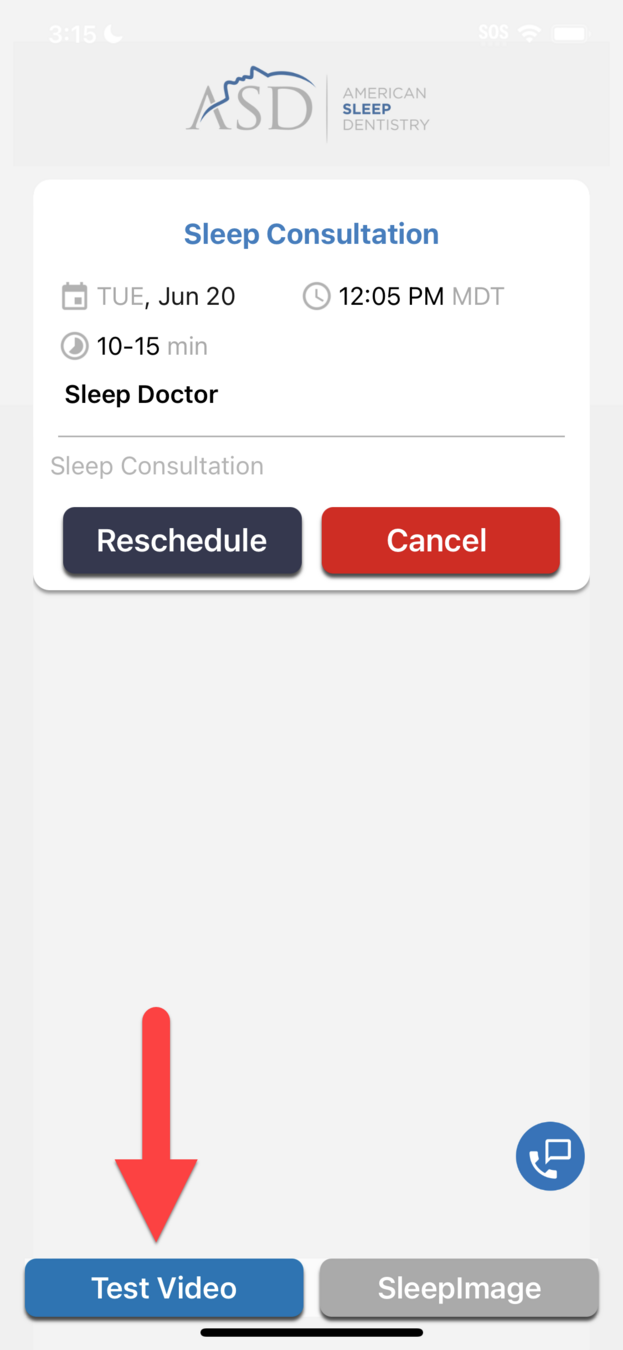
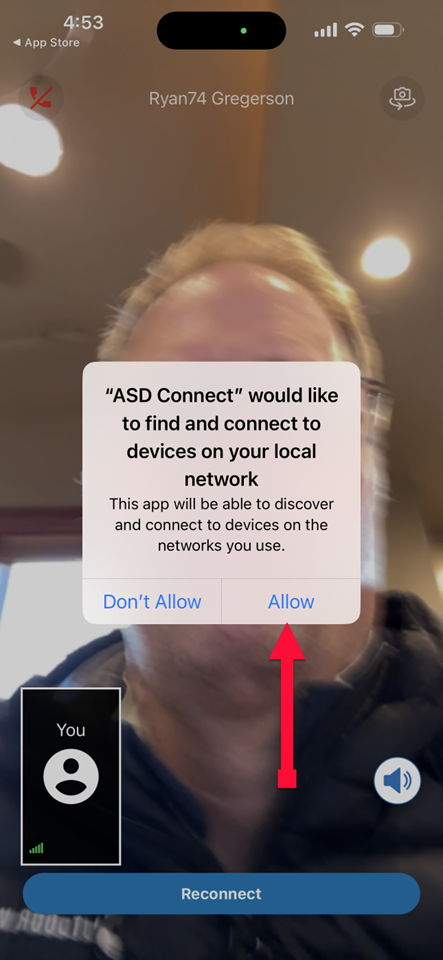
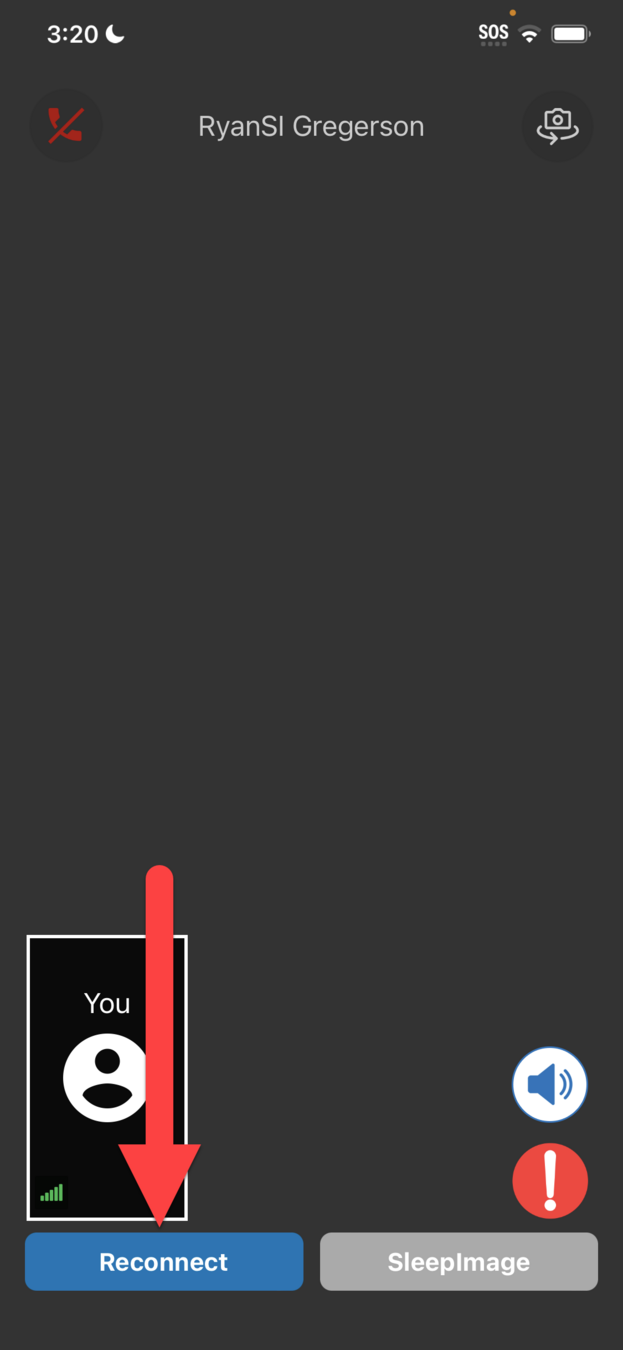
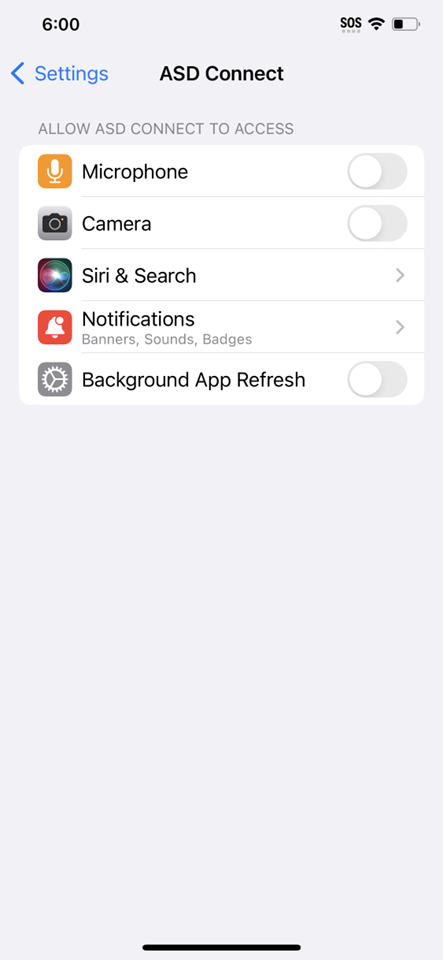
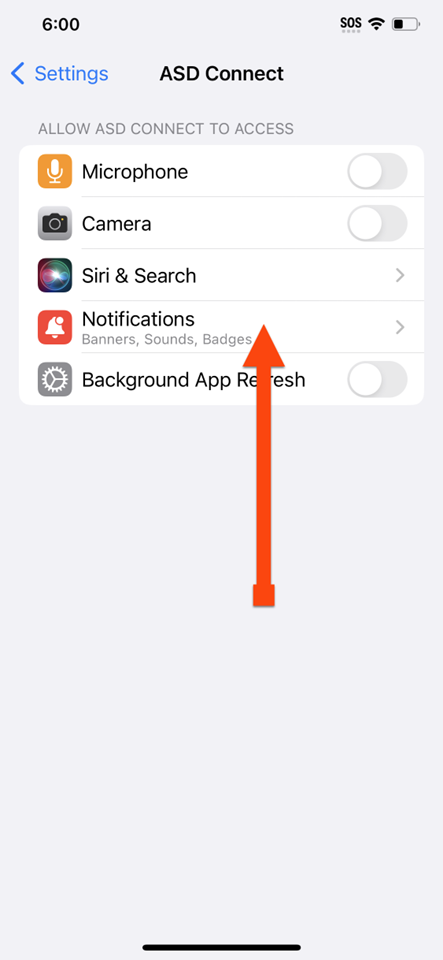
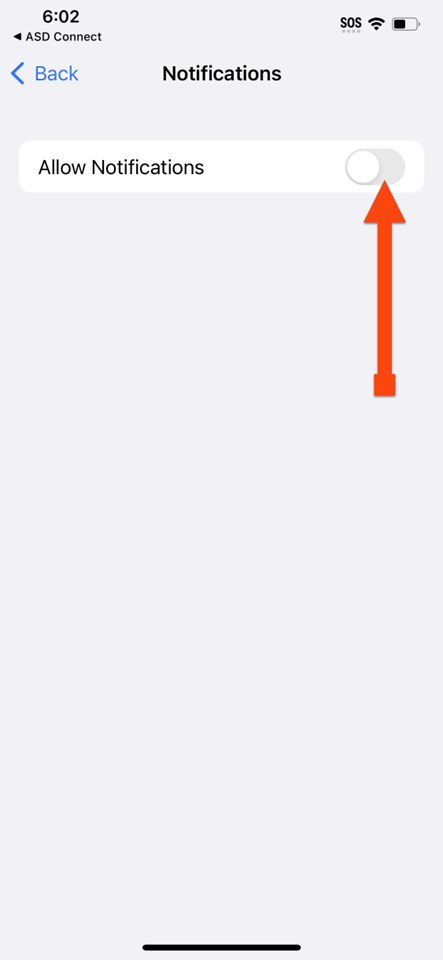
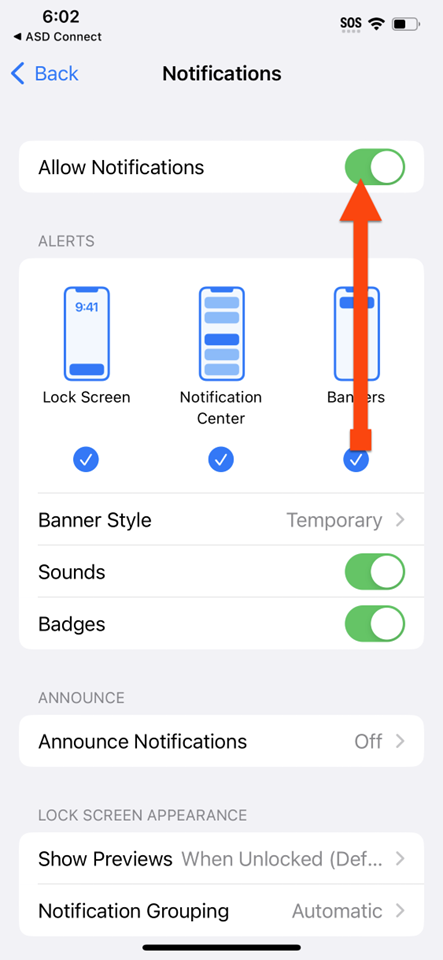
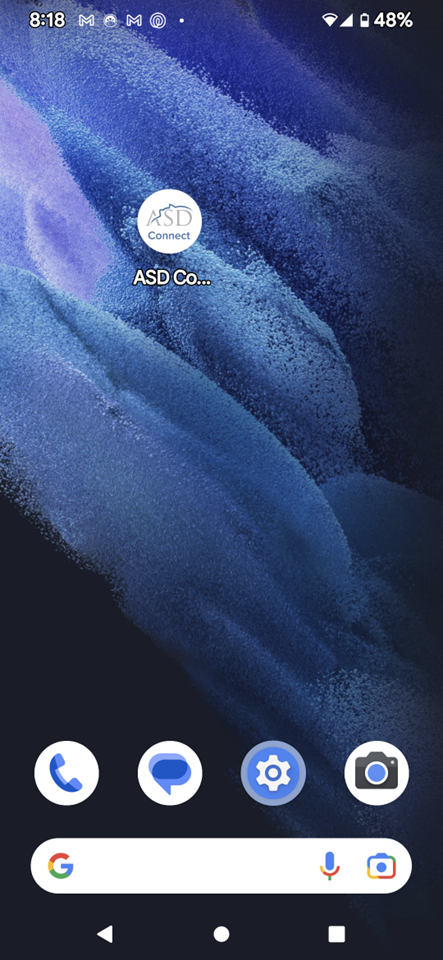
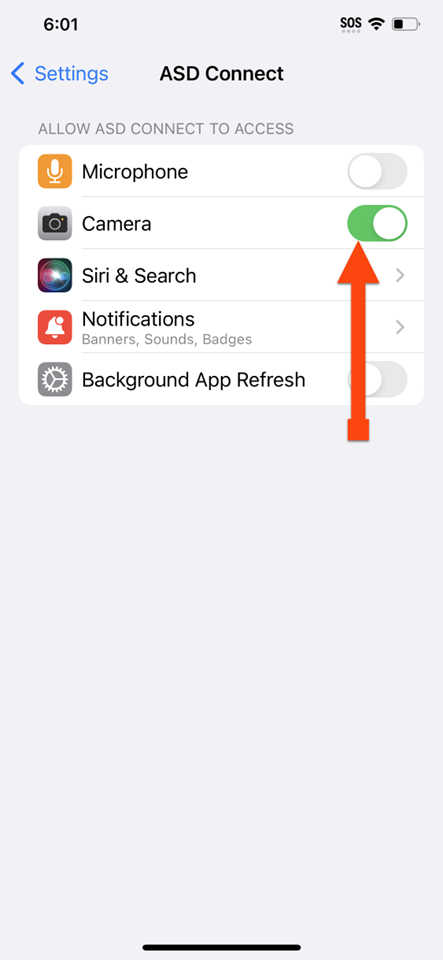
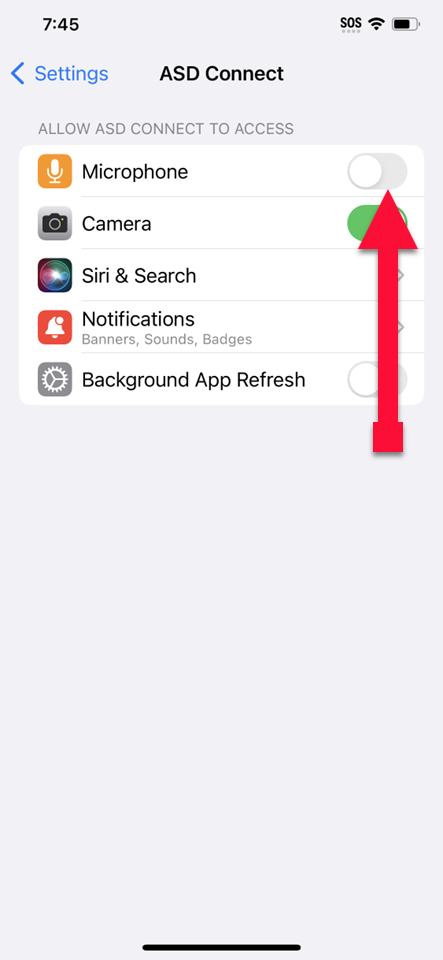
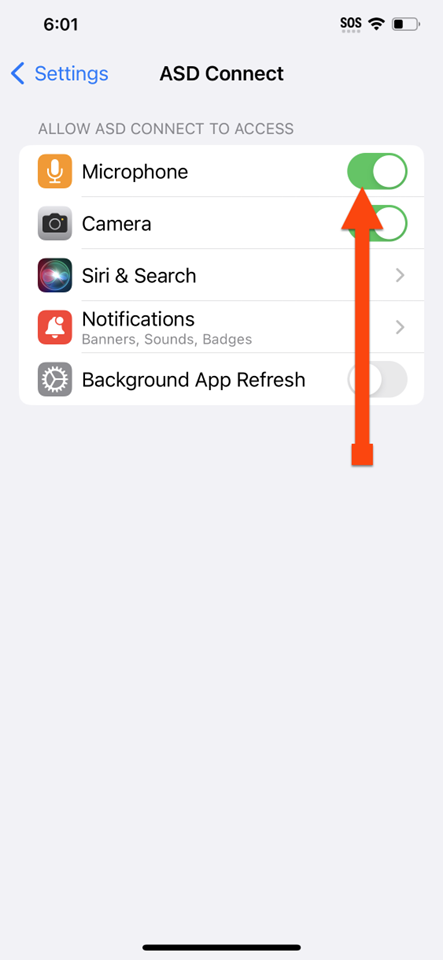
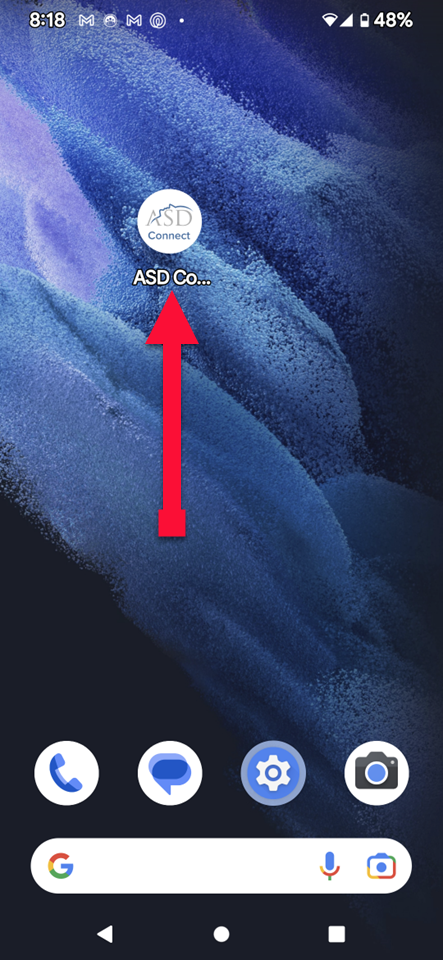
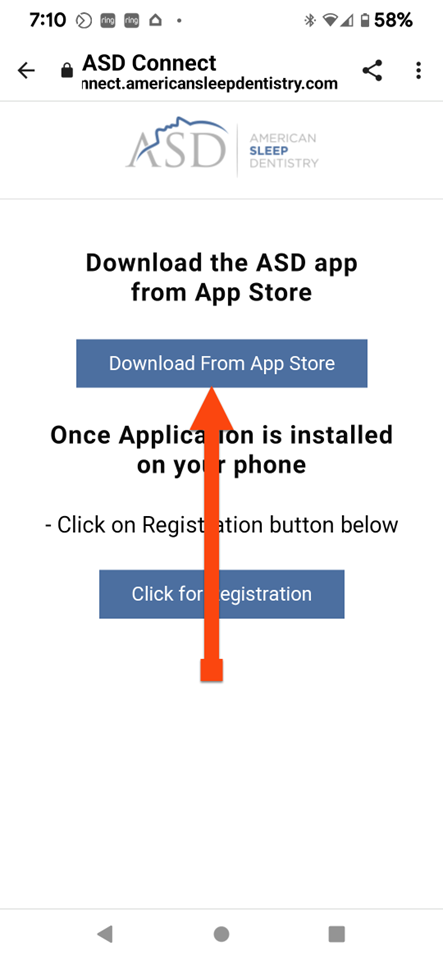
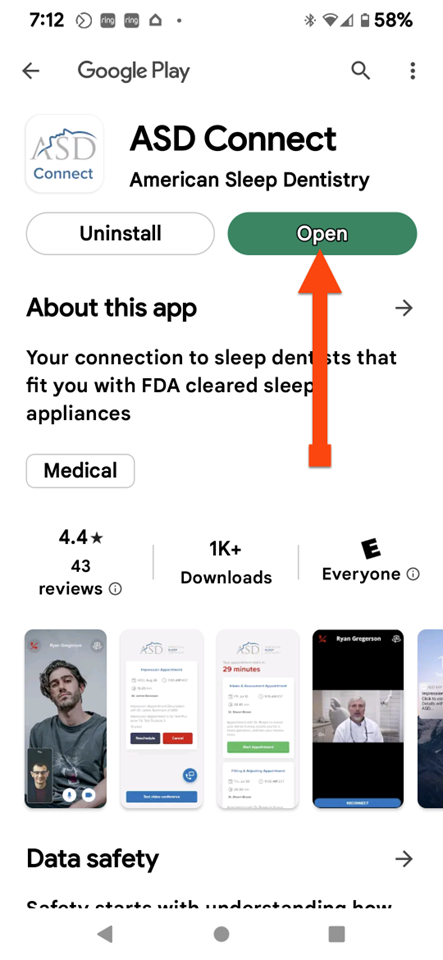
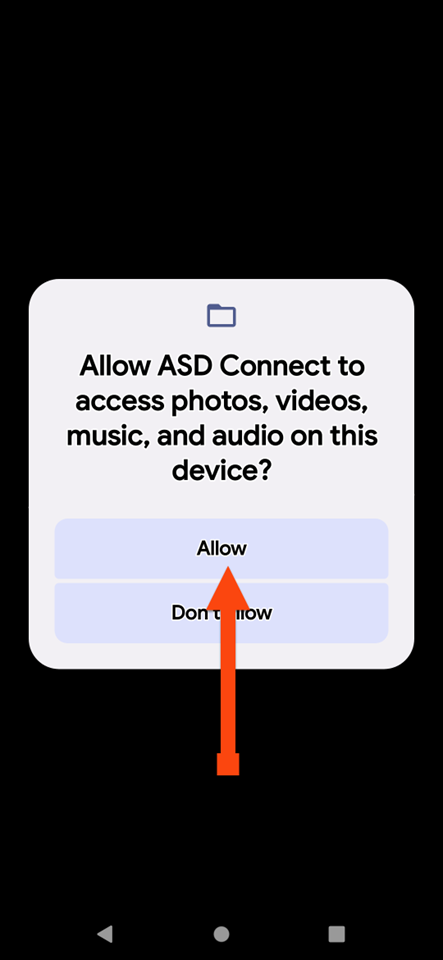
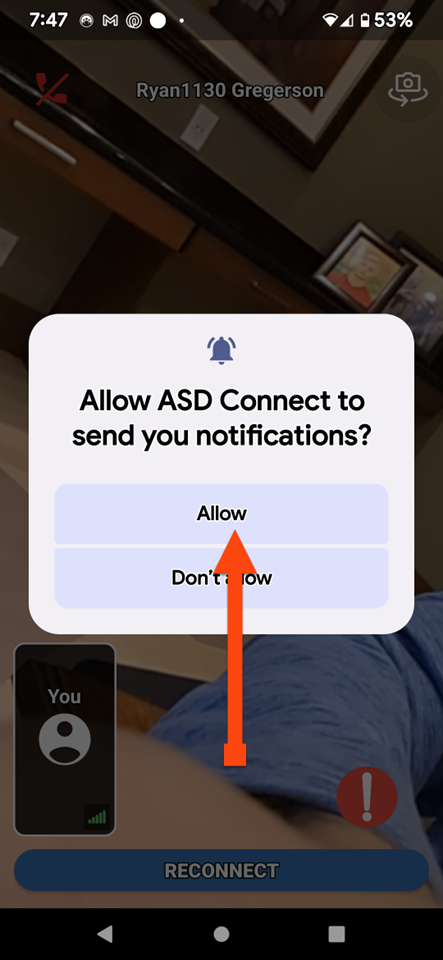
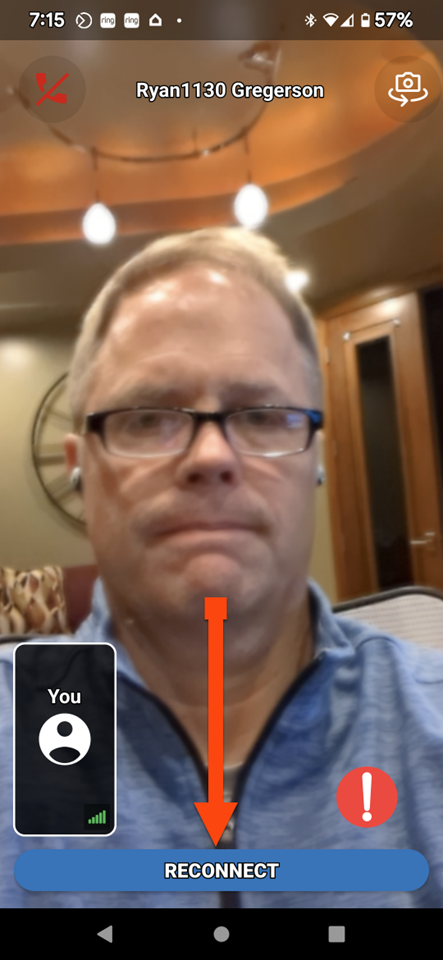
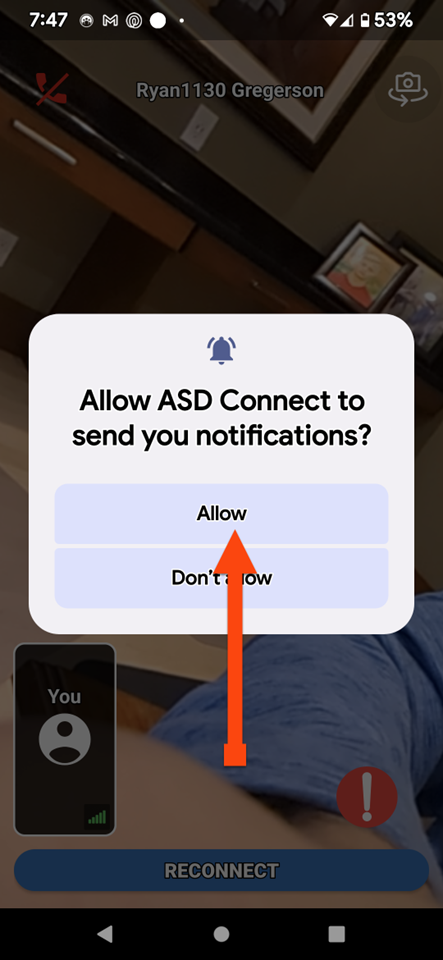
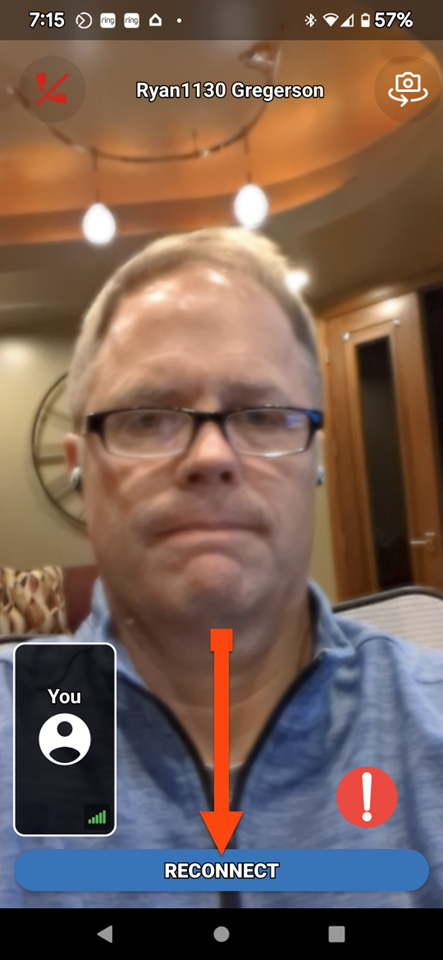
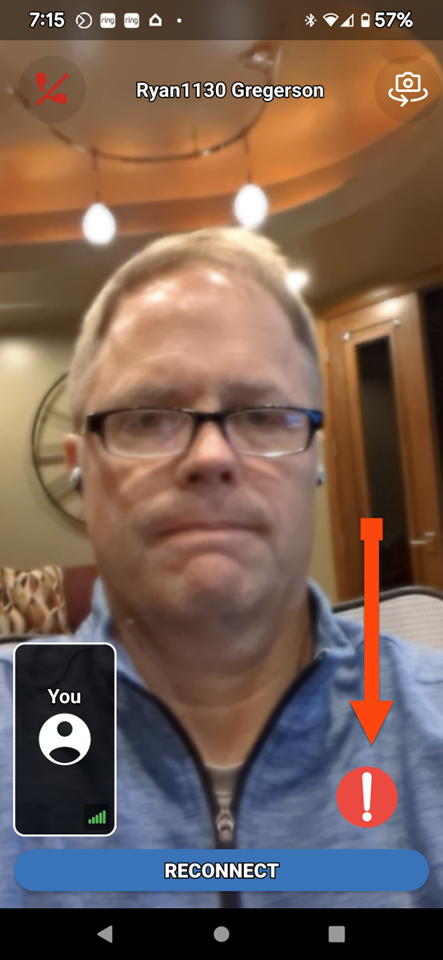
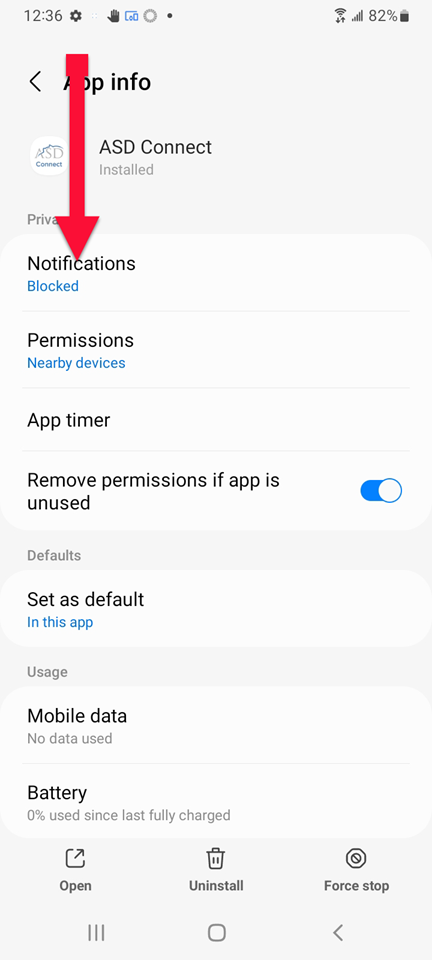
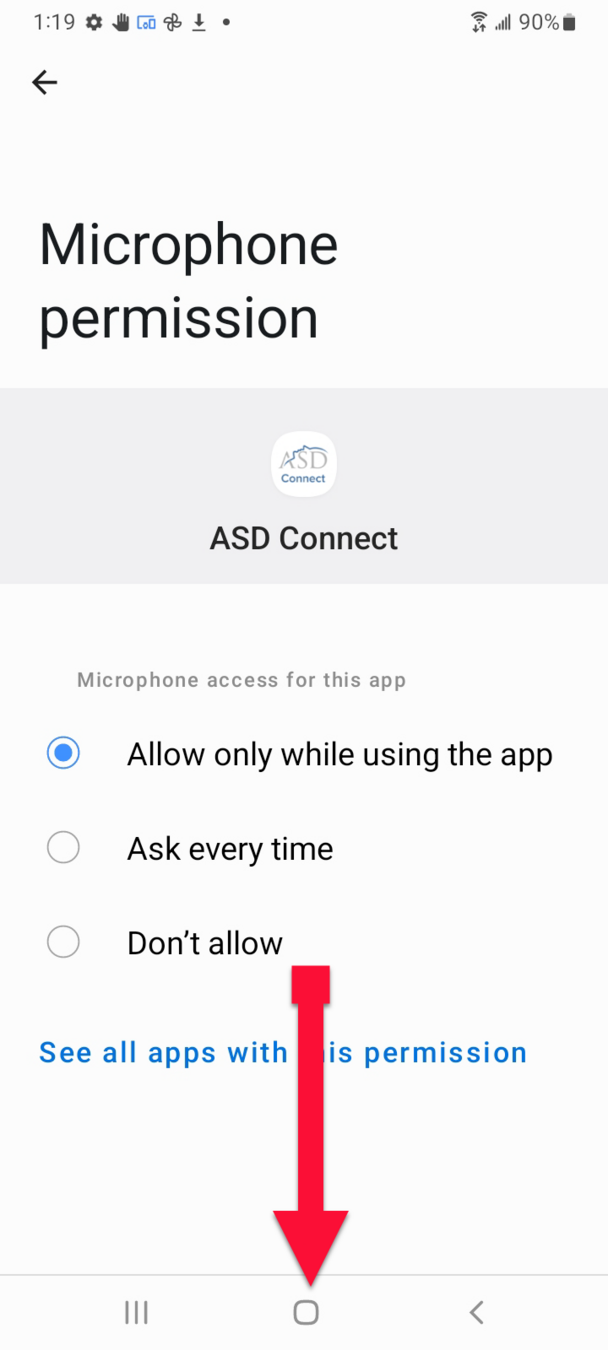
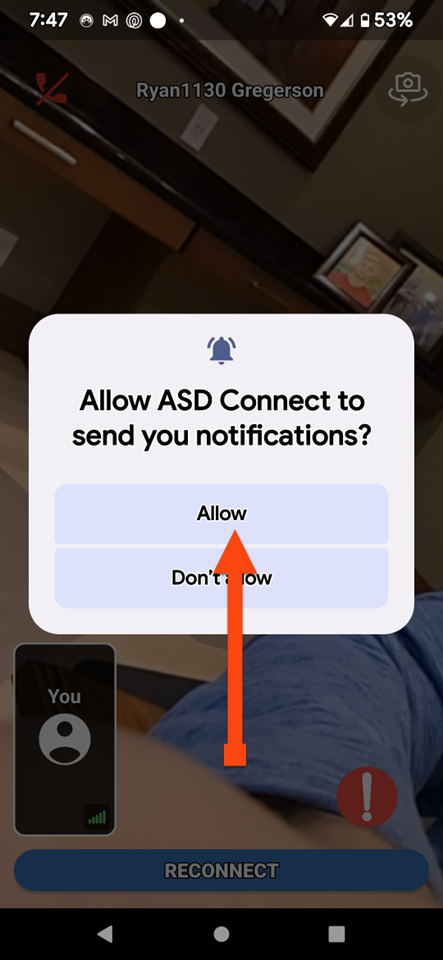
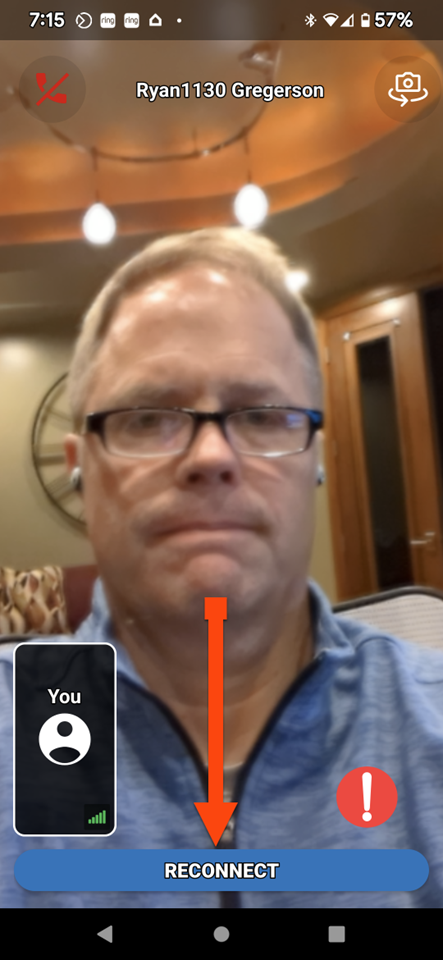
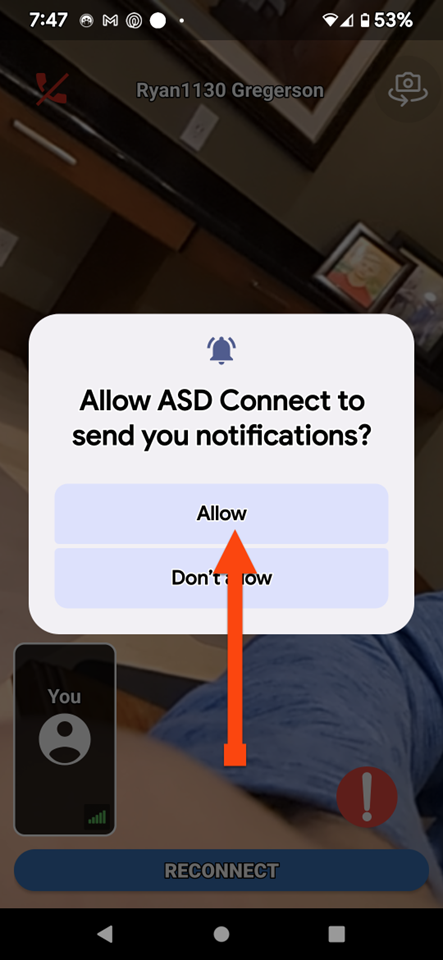
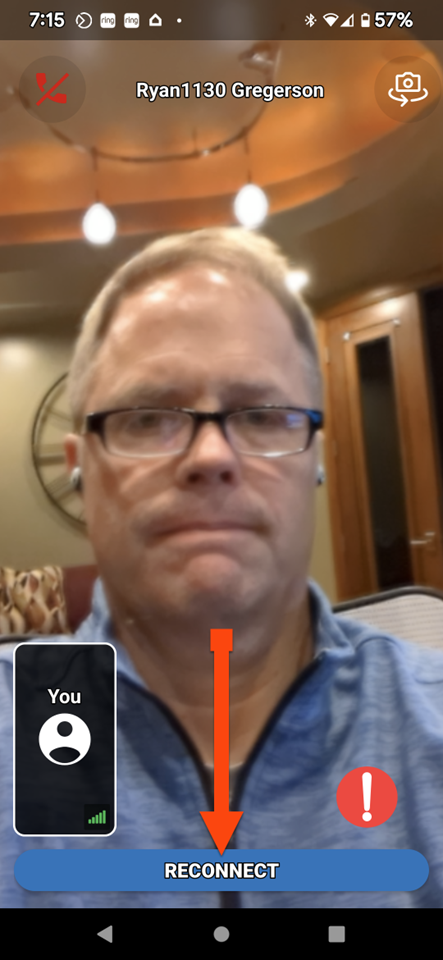
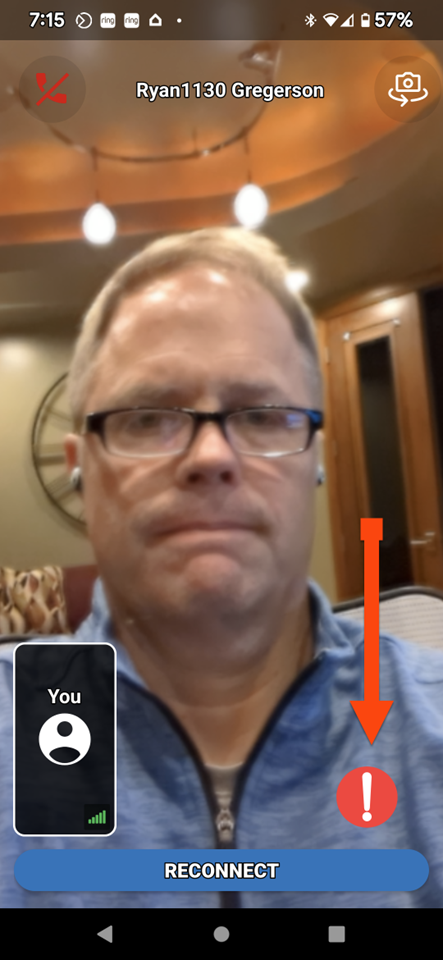
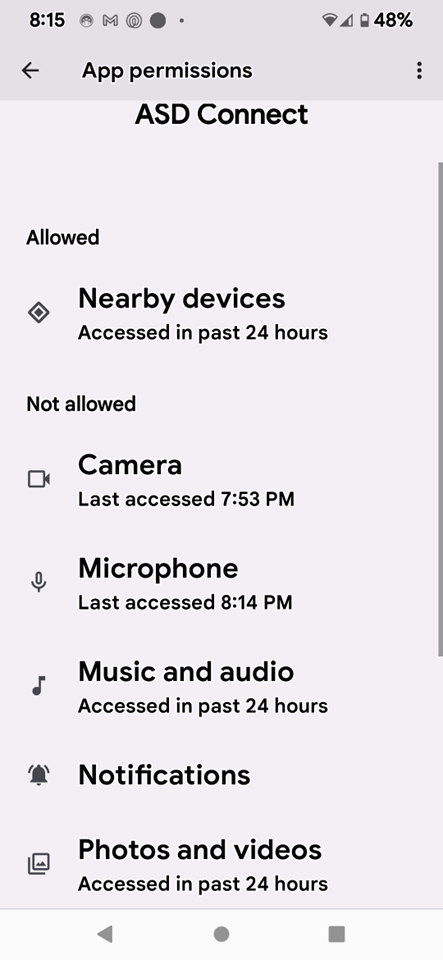
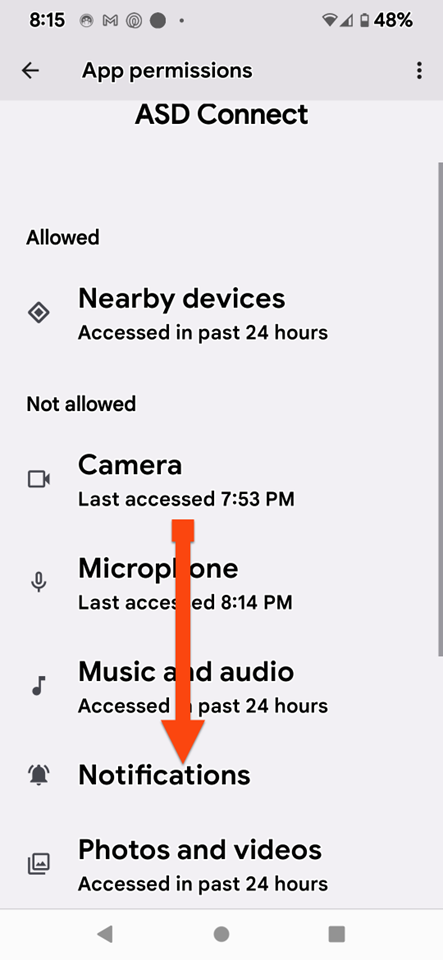
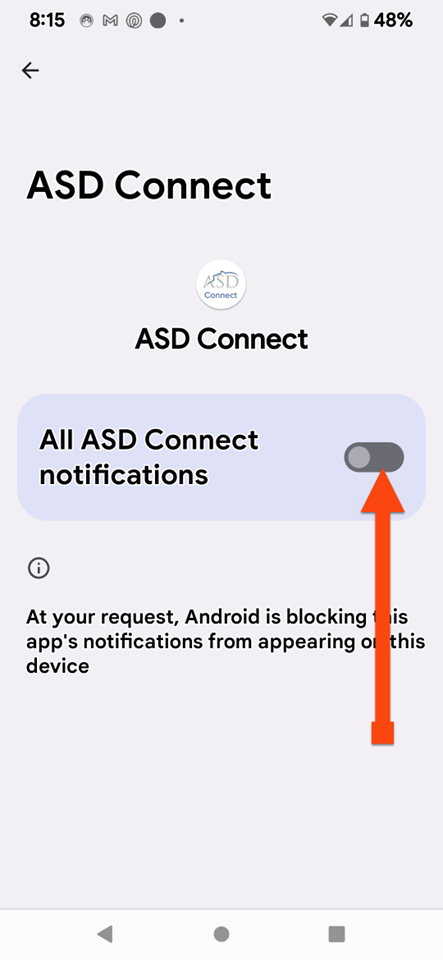
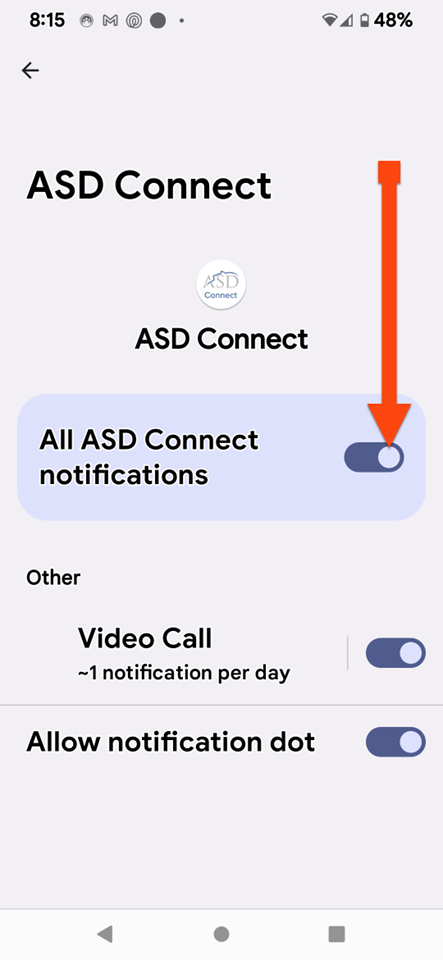
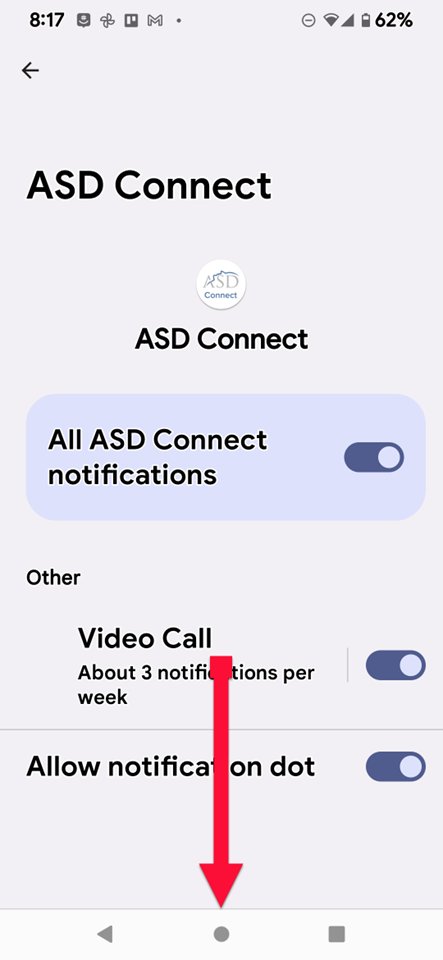
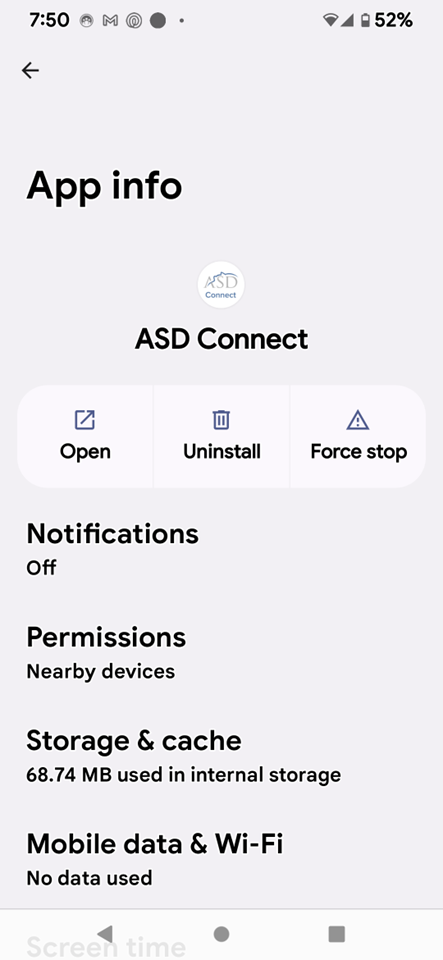
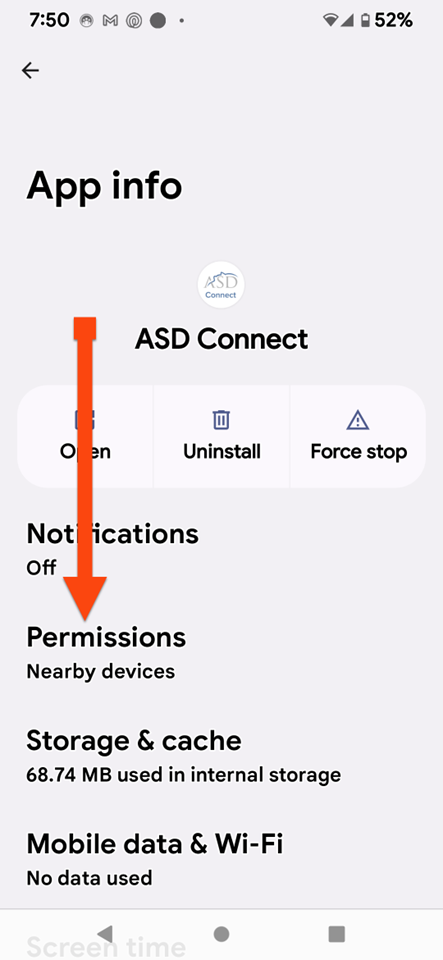
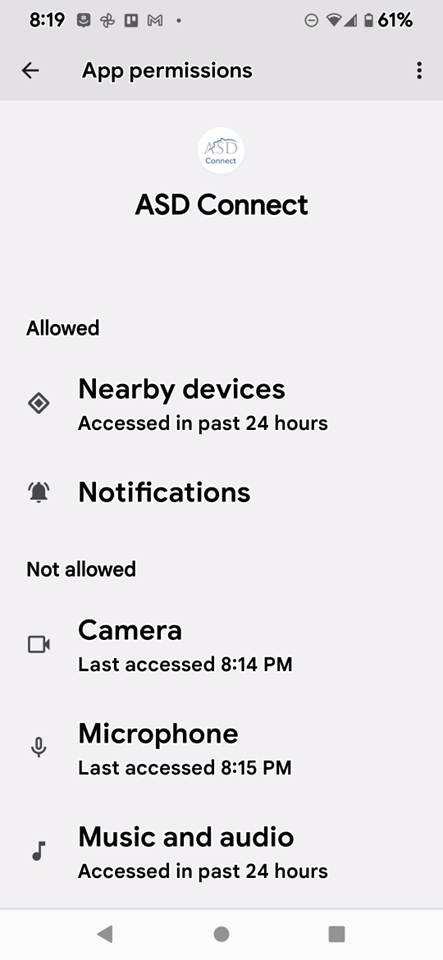
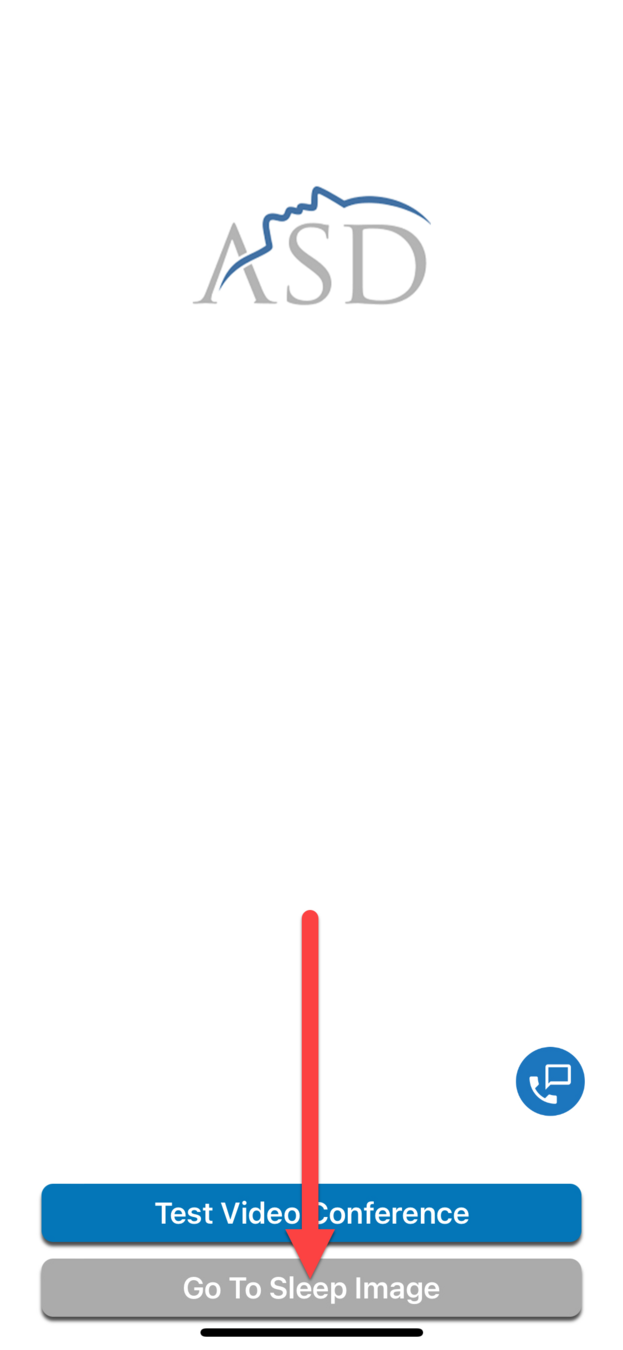
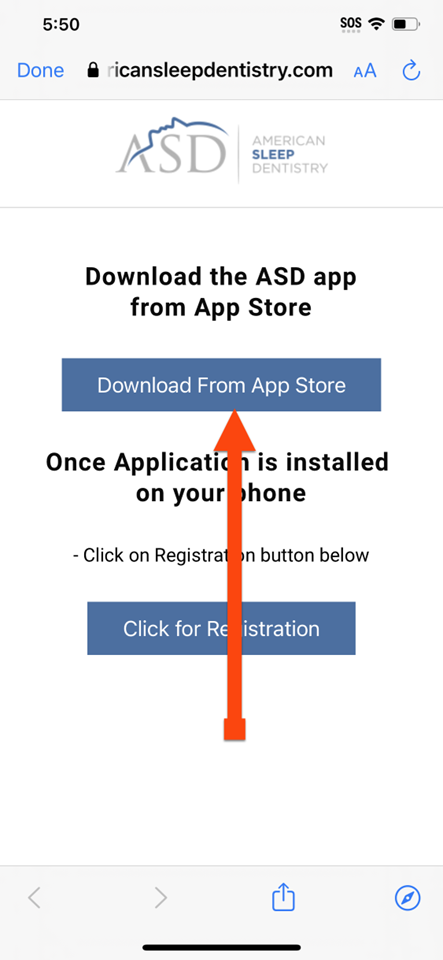
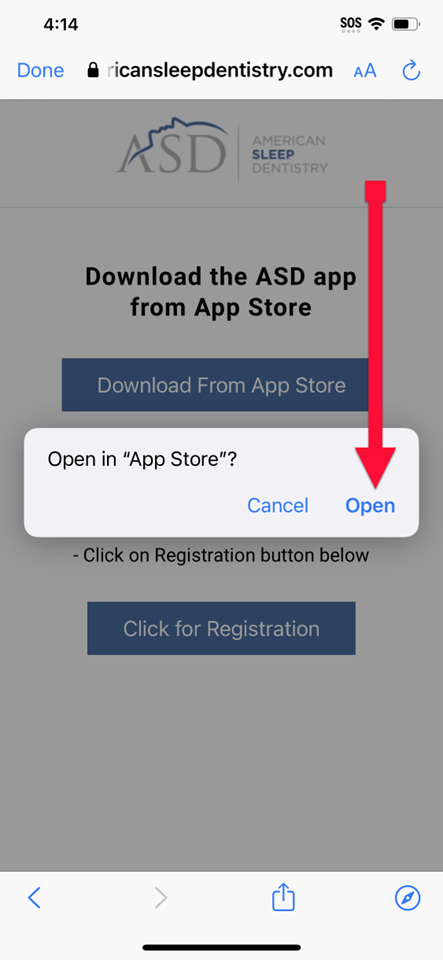
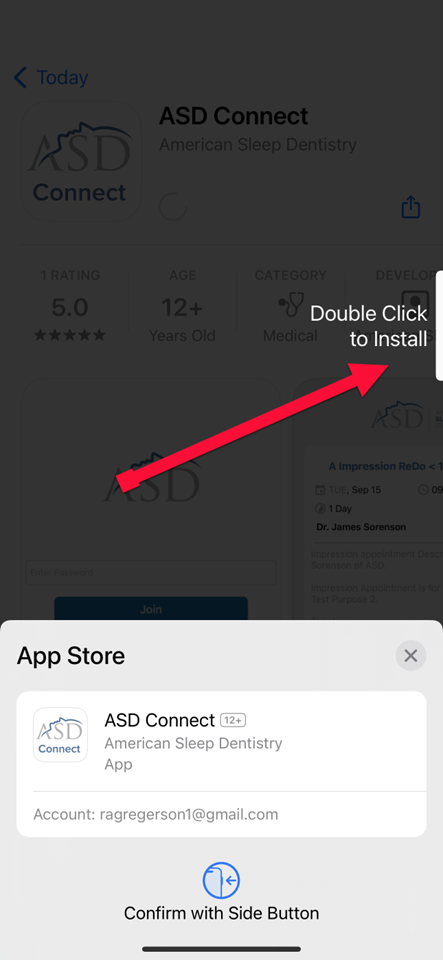
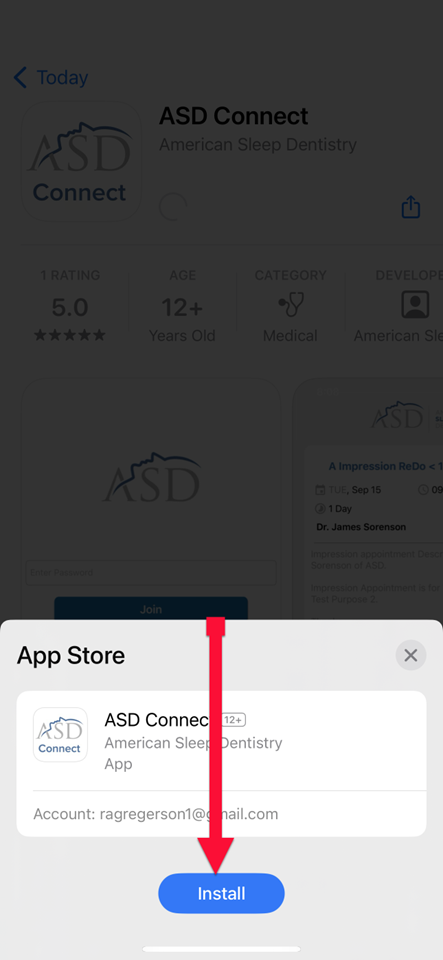
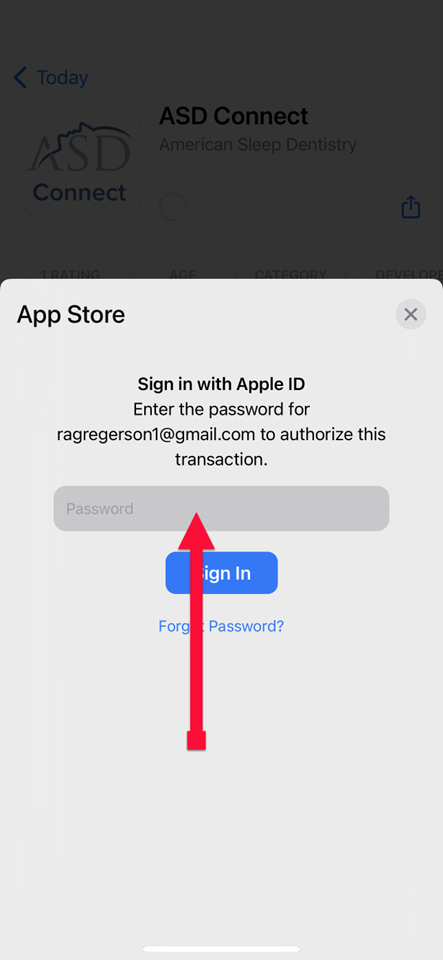
Keep the ASD Connect App Open
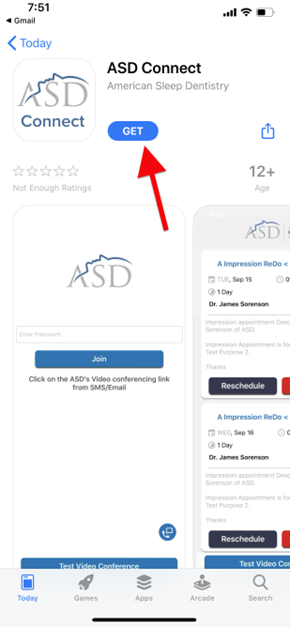
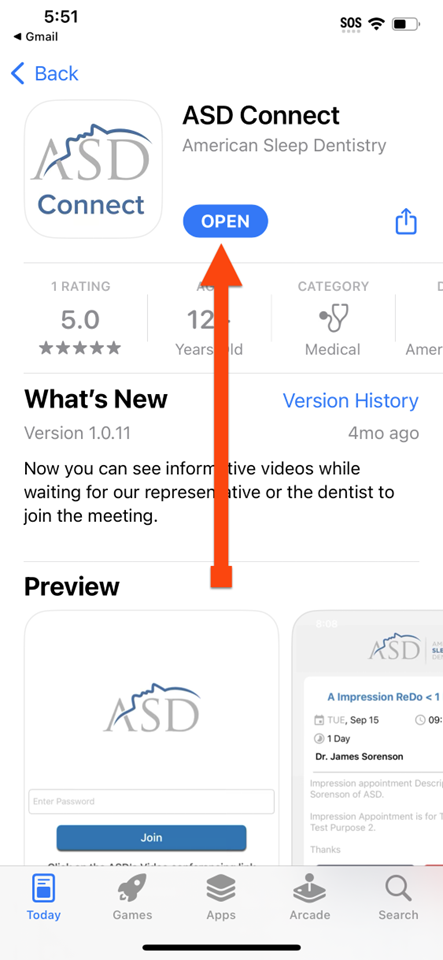
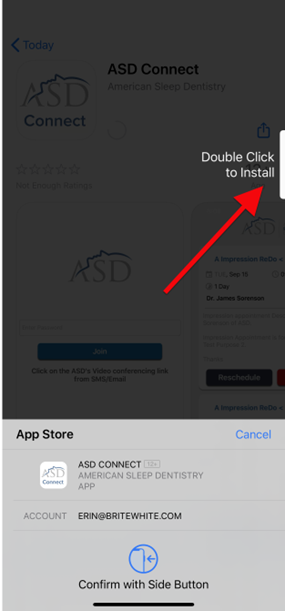
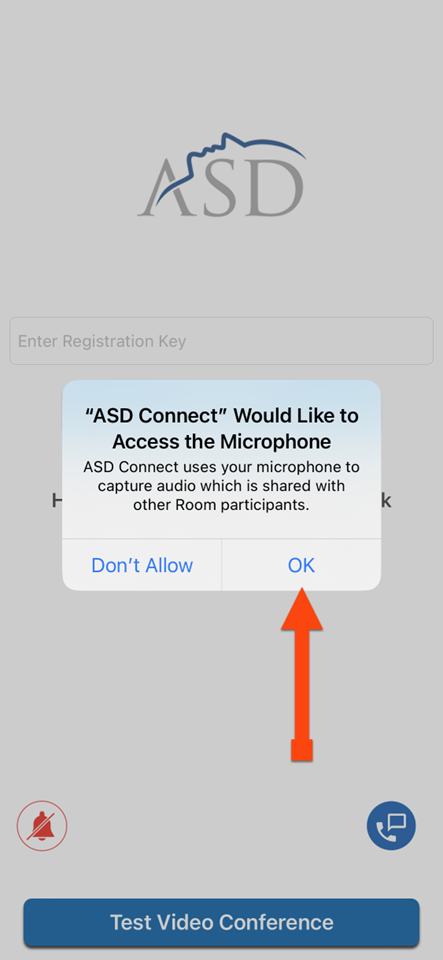
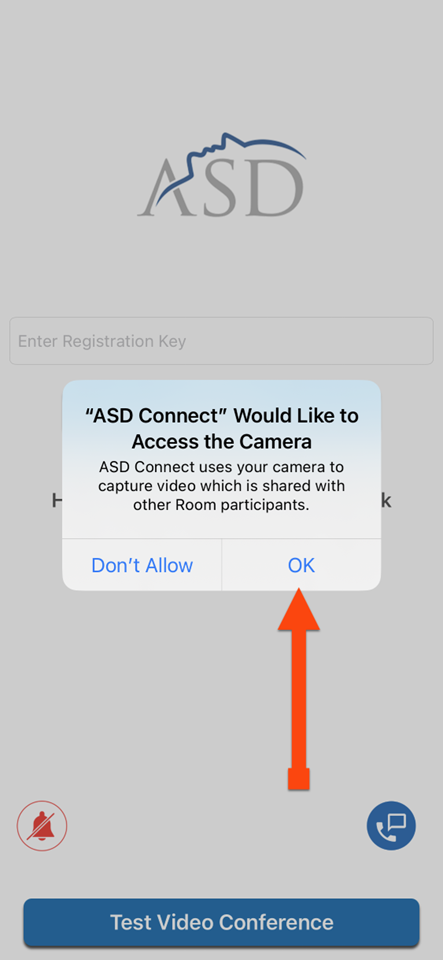
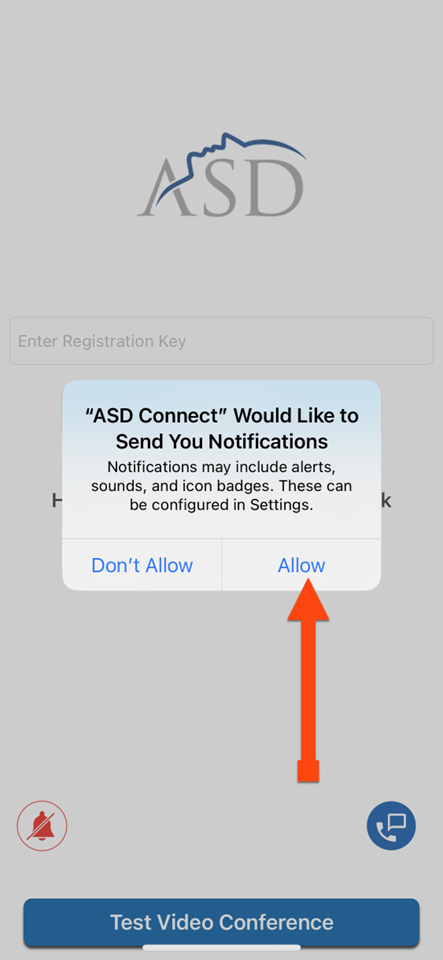
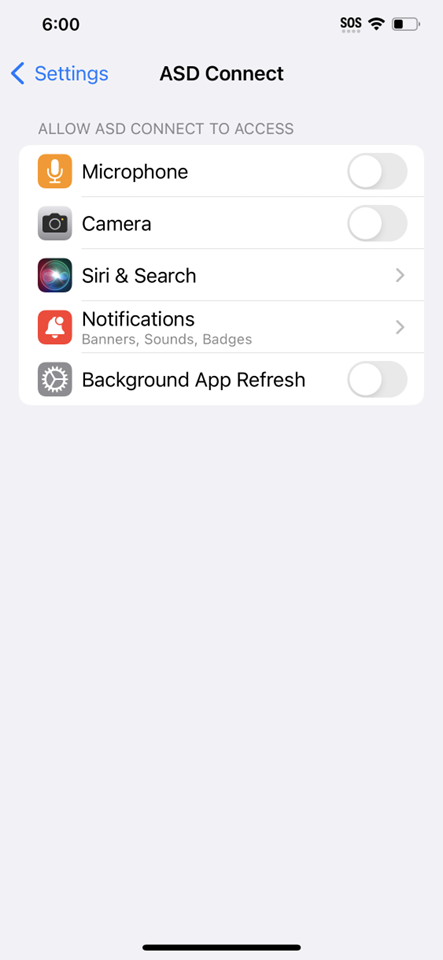
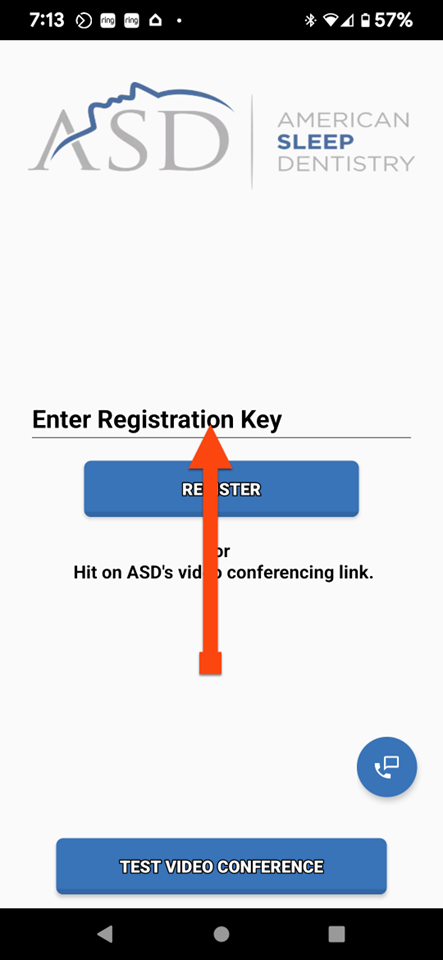
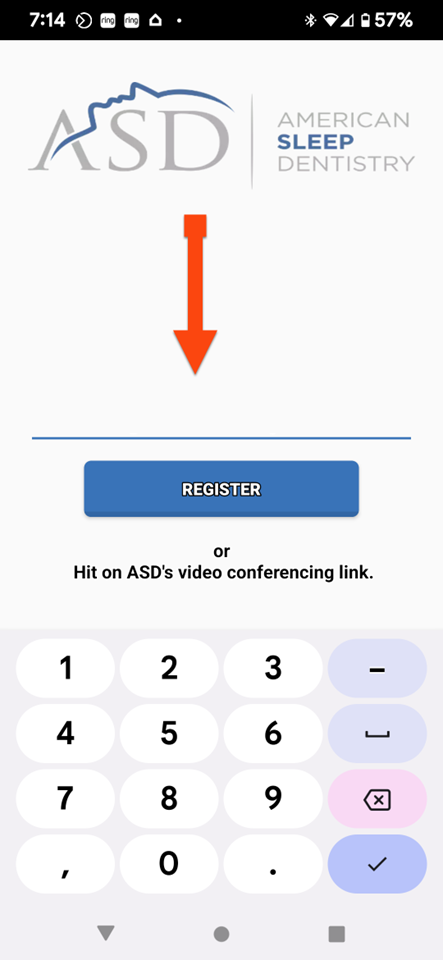
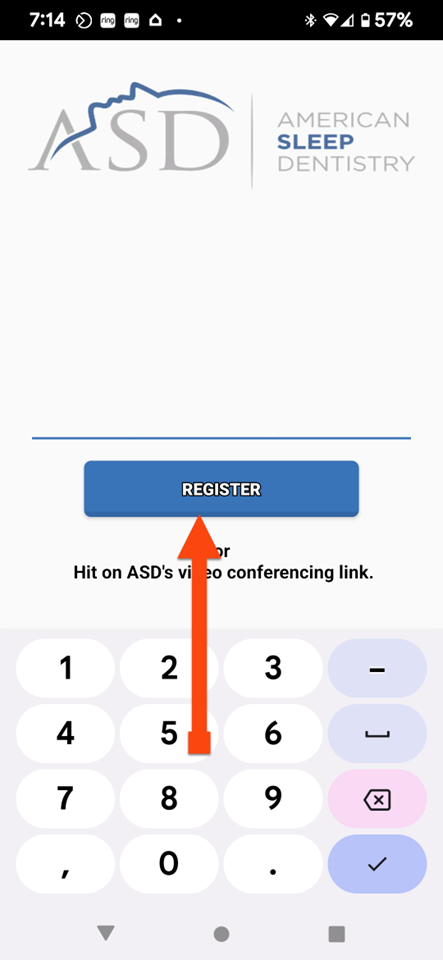
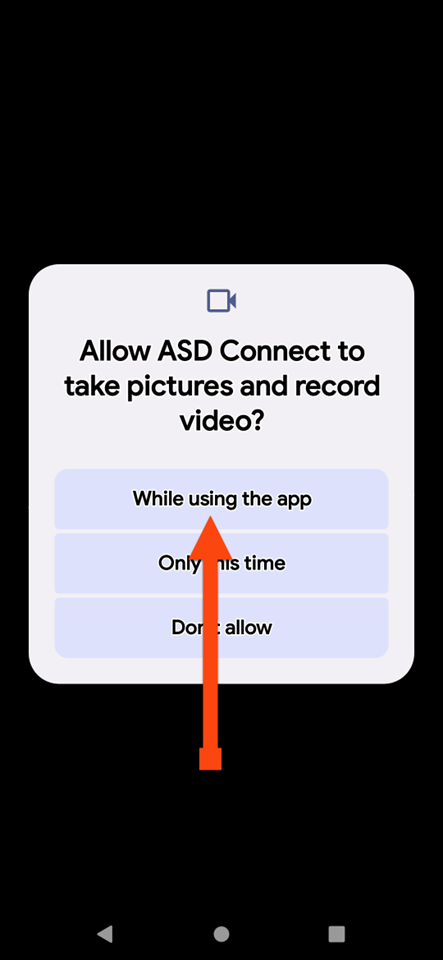
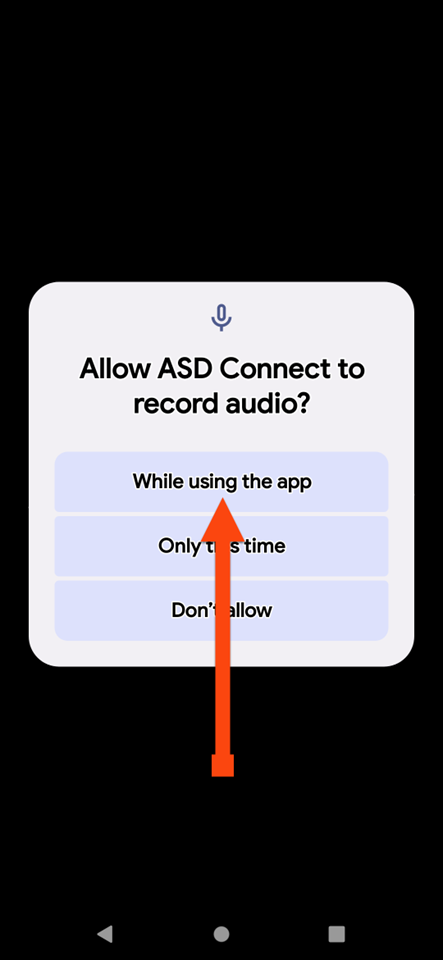
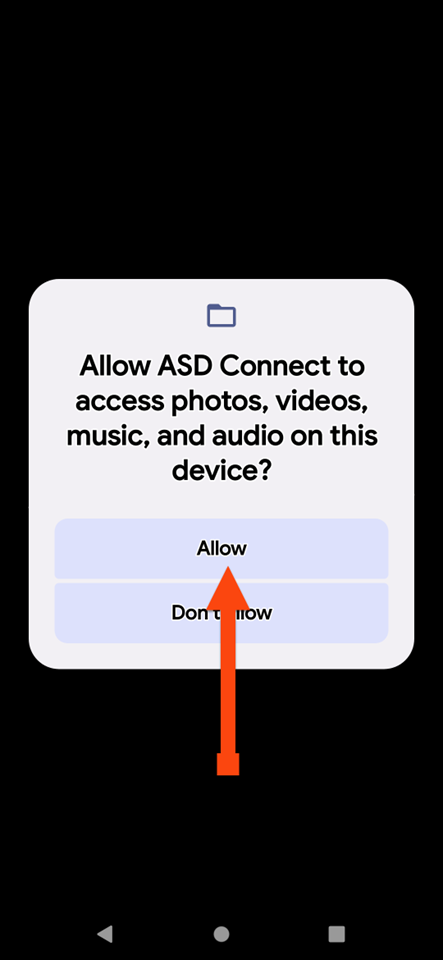
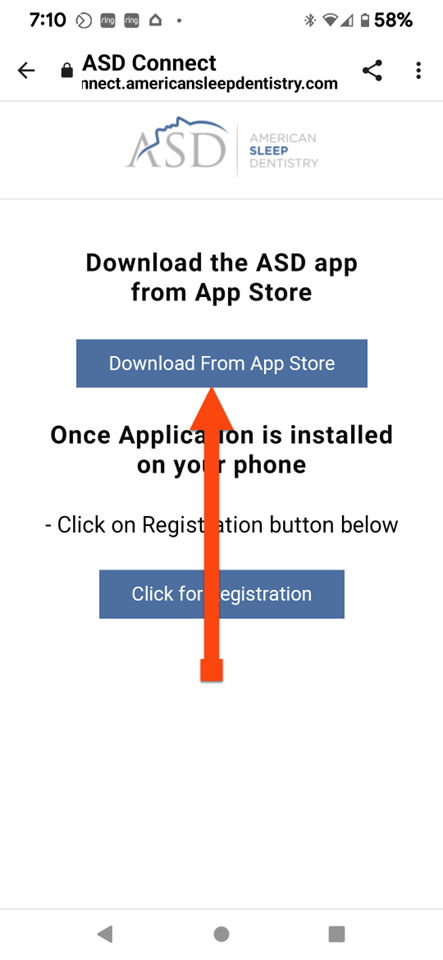
ASD CONNECT

ASD CONNECT
ASD CONNECT
ASD CONNECT
STOP BANG
Stop Bang Questionnaire
STOP BANG

STOP BANG

STOP BANG

STOP BANG

STOP BANG
STOP BANG

STOP BANG

STOP BANG
APPOINTMENT DATE & TIME
Date:
Time:
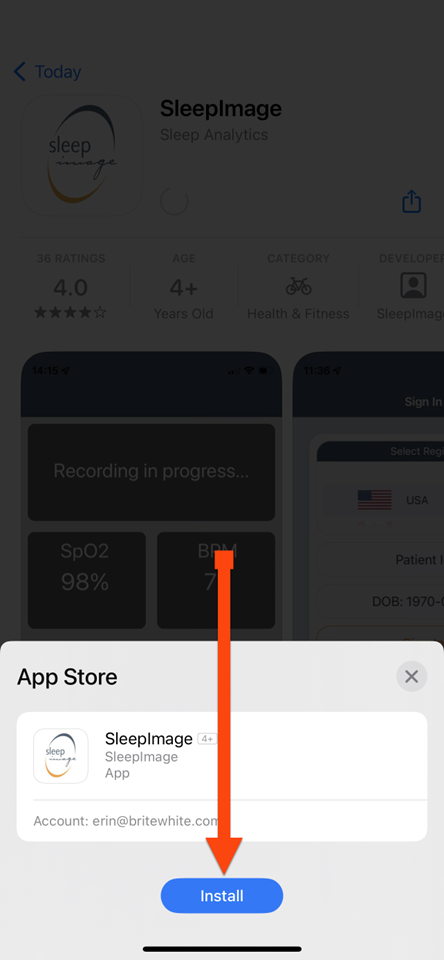
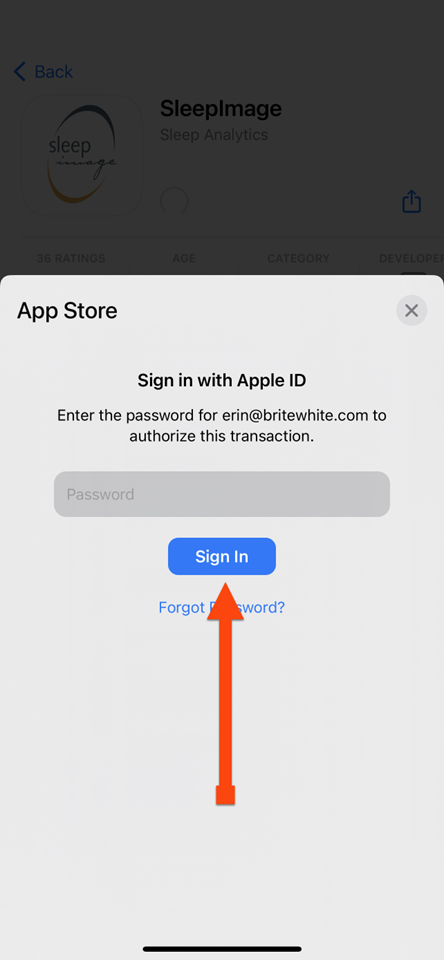
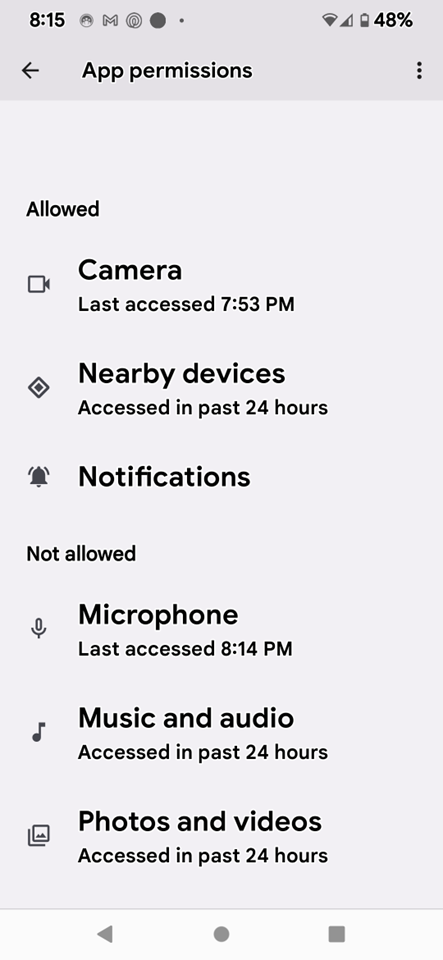
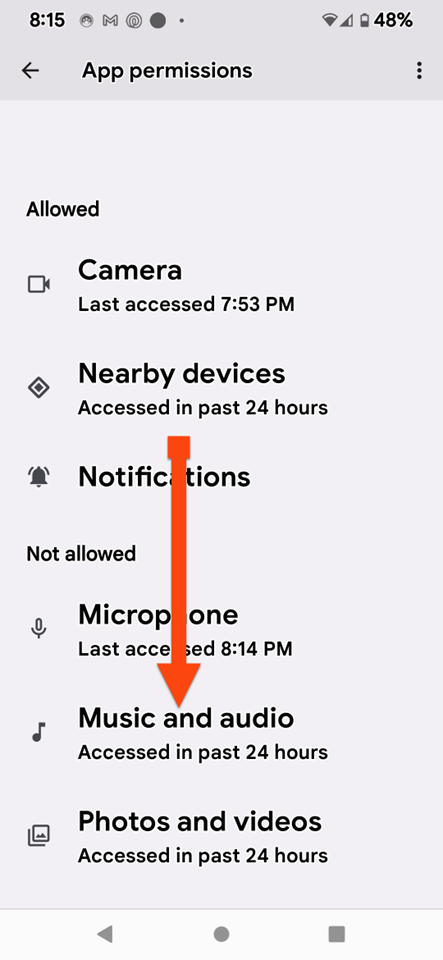
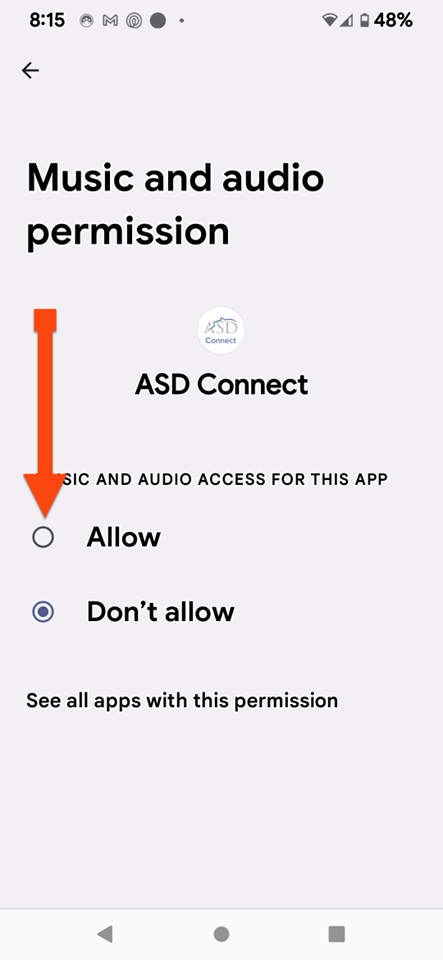
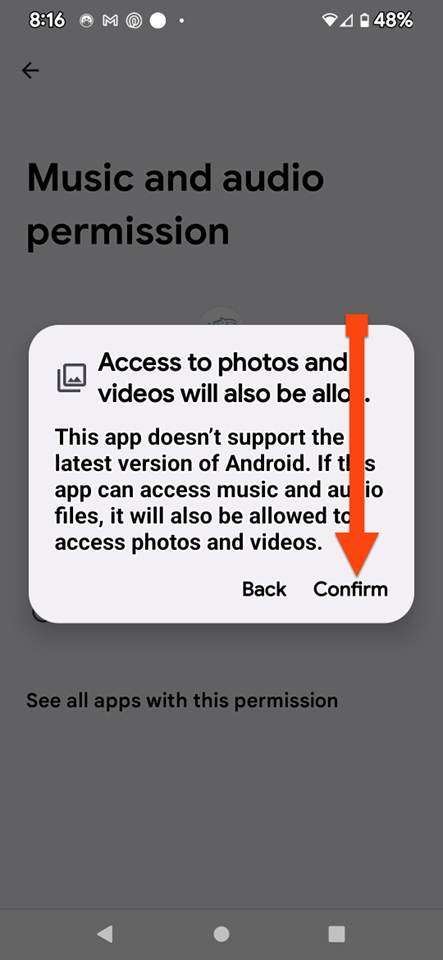
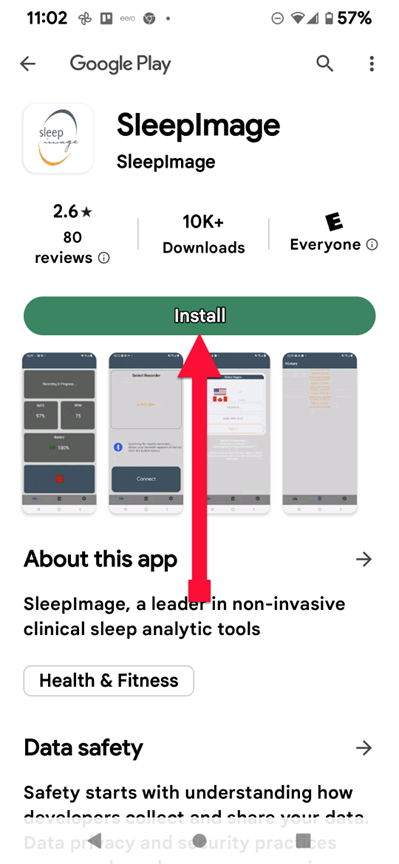
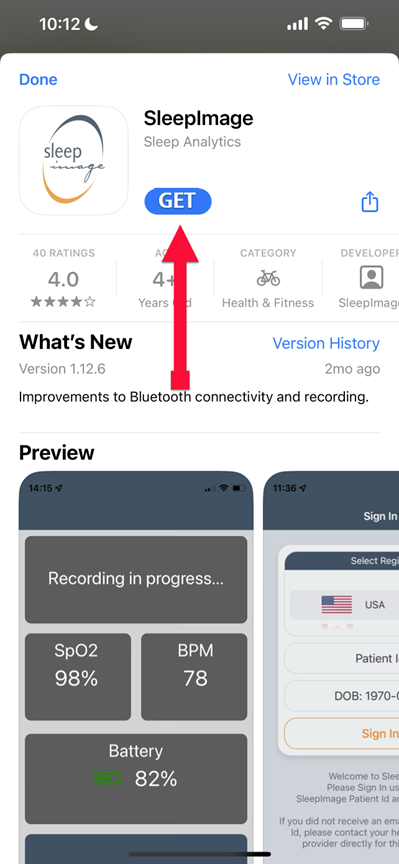
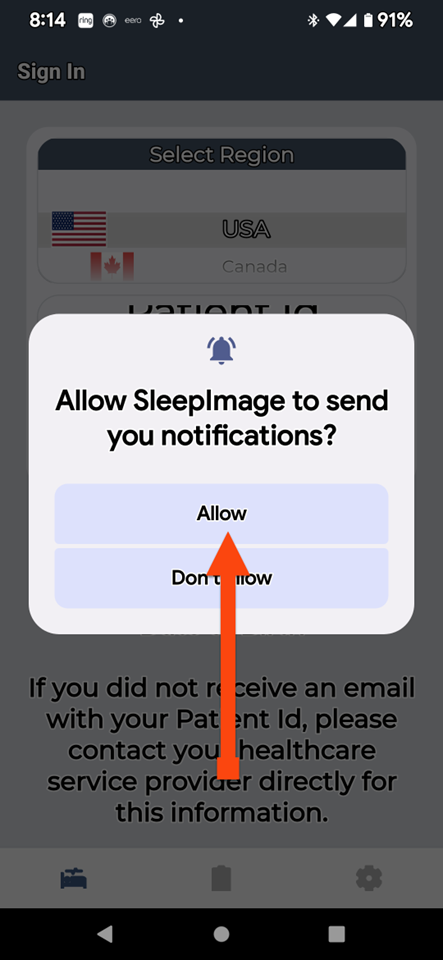
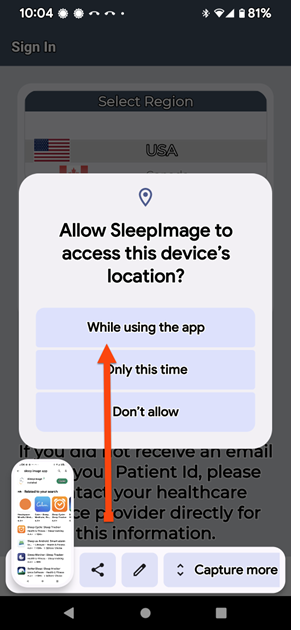
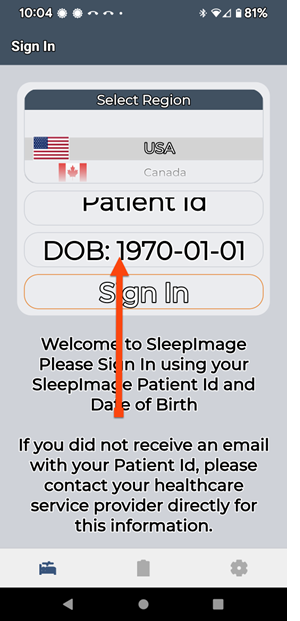
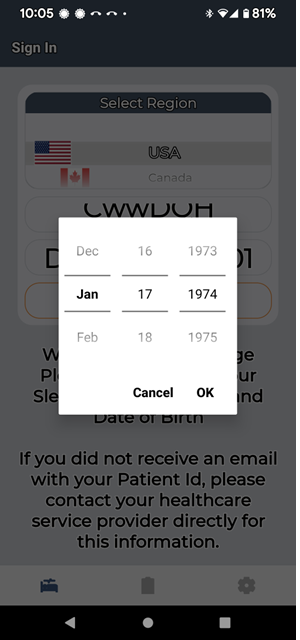
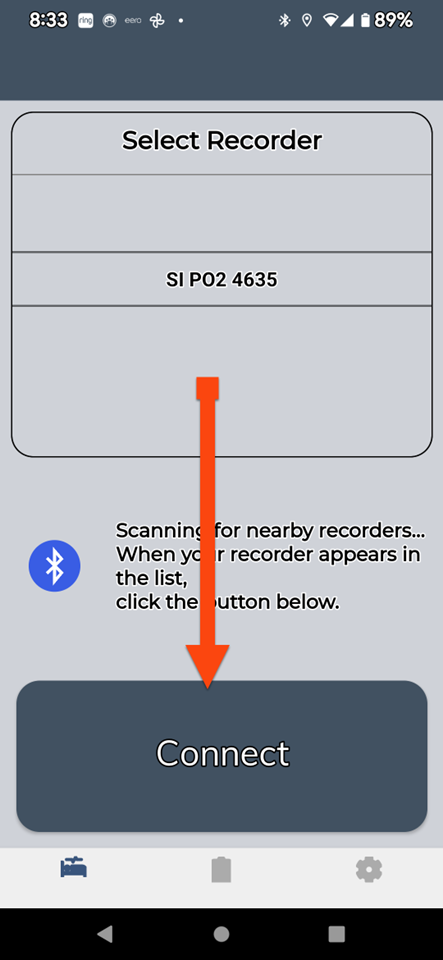
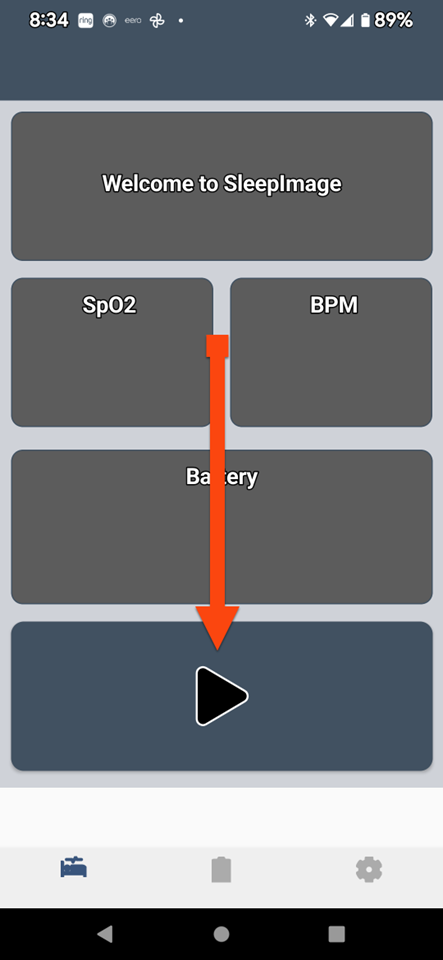
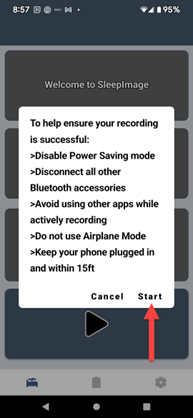
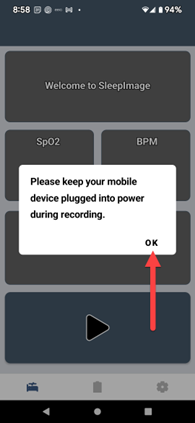
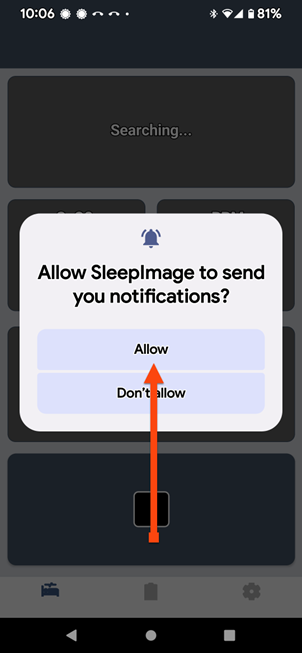
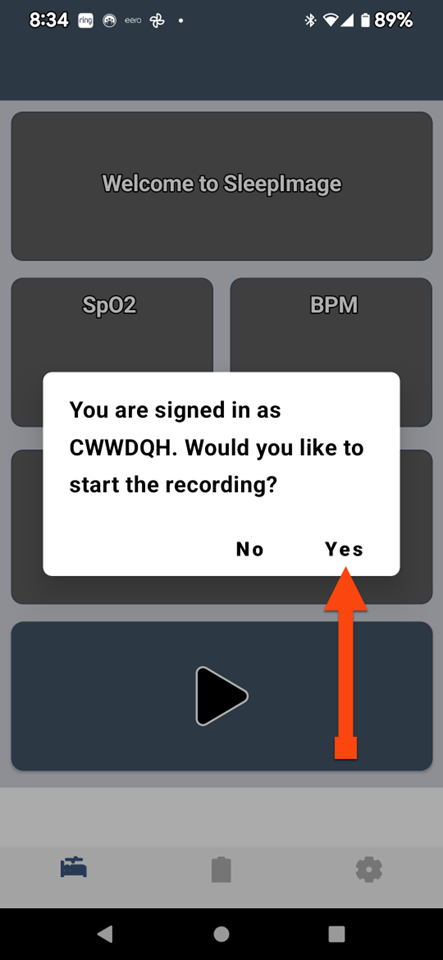
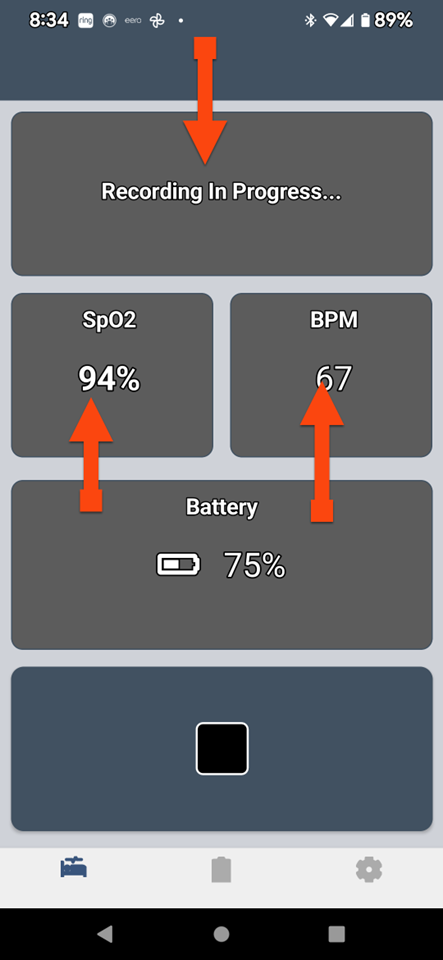
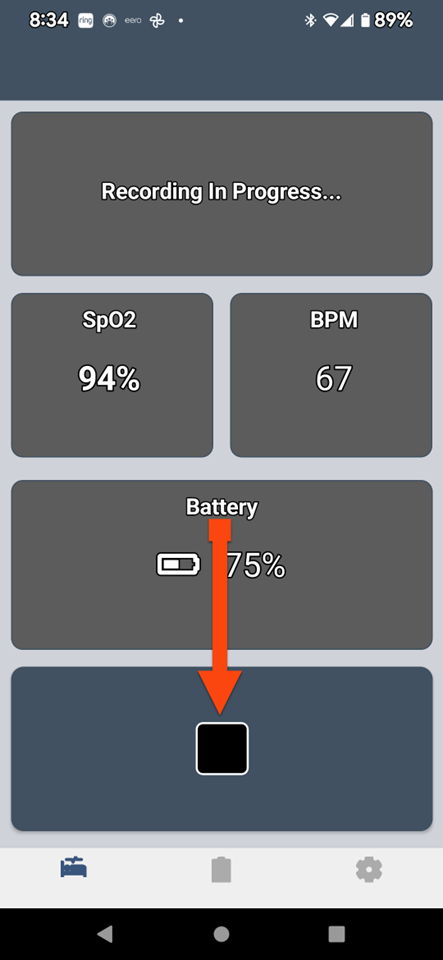
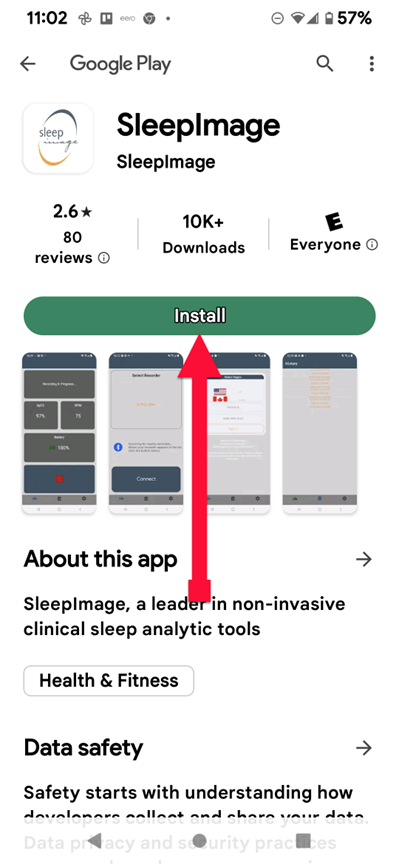
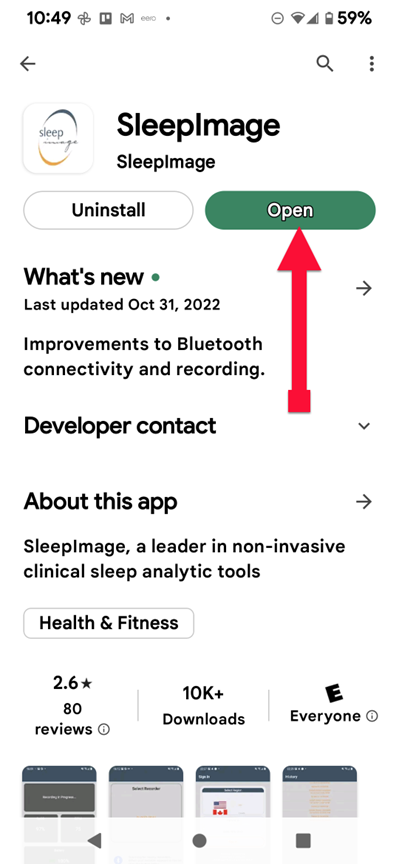
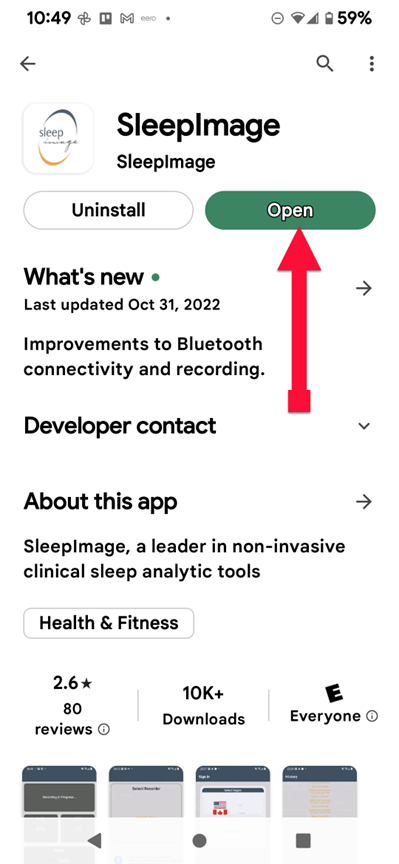
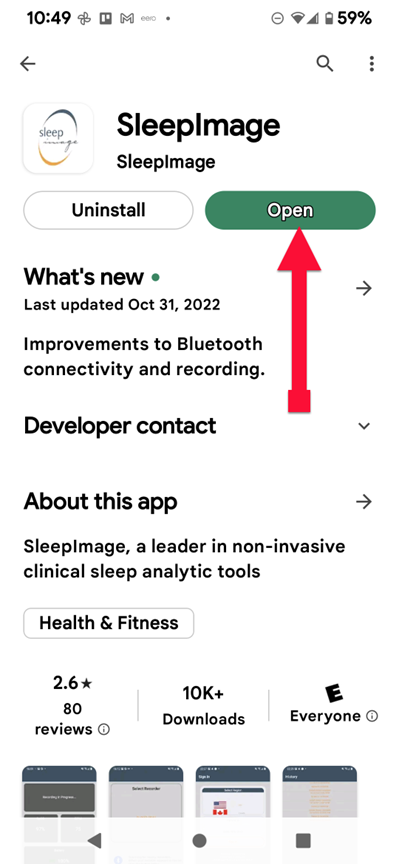
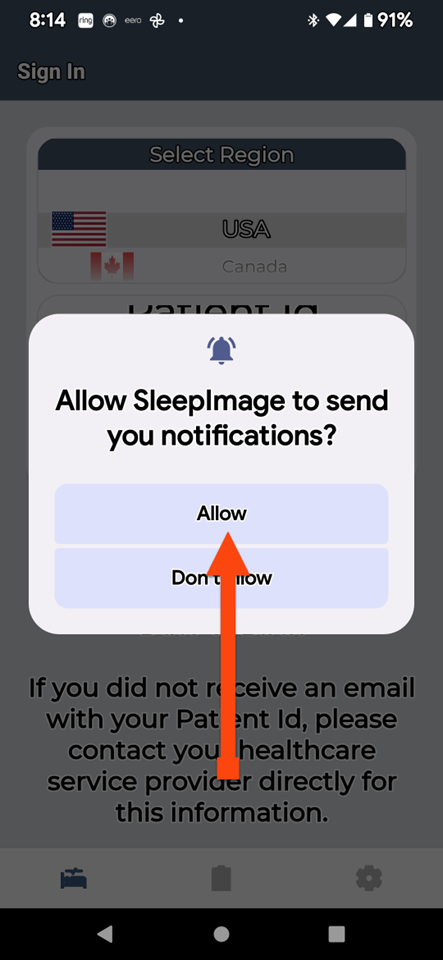
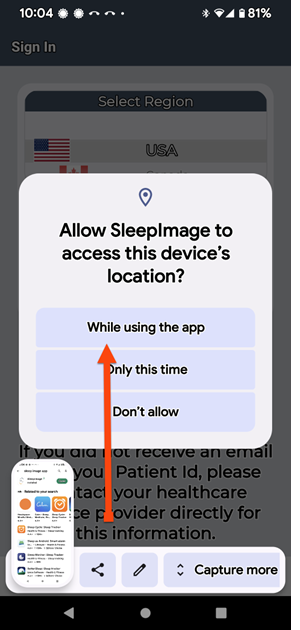
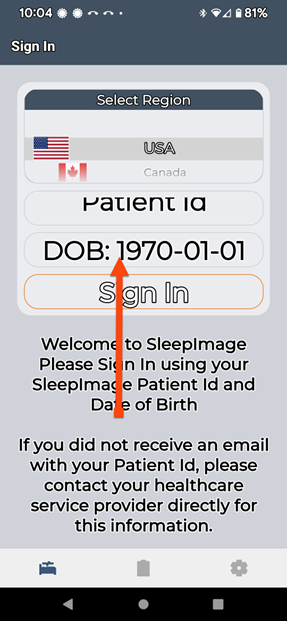
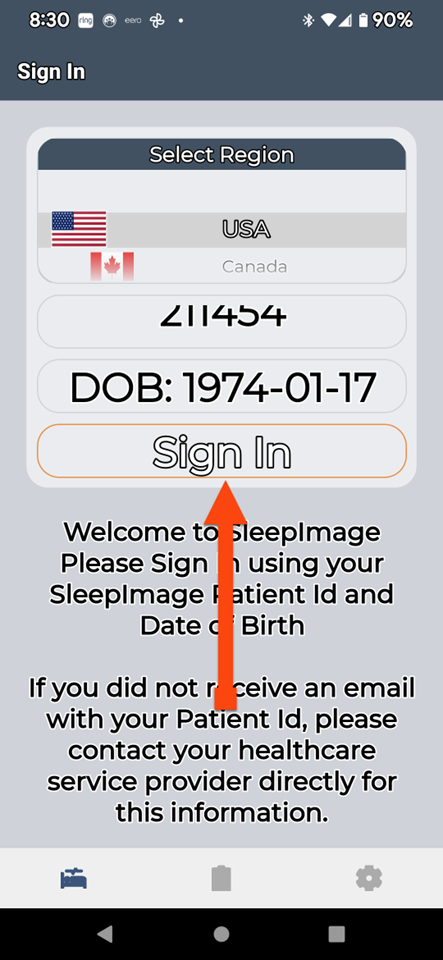
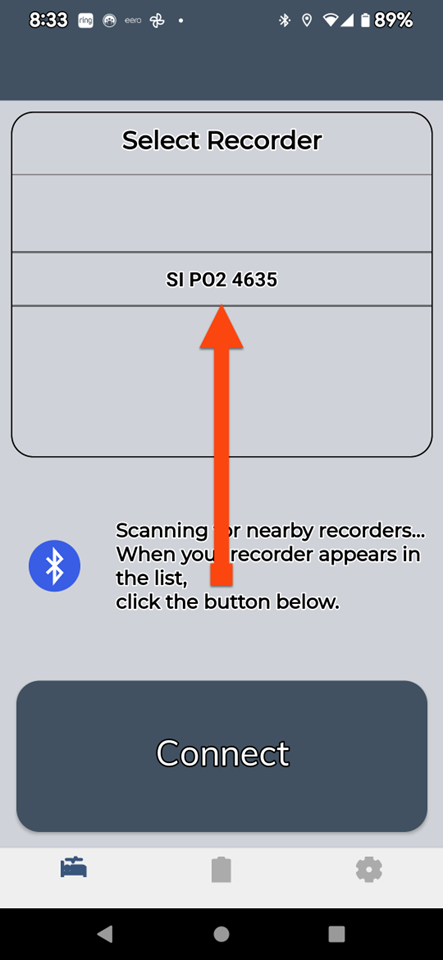
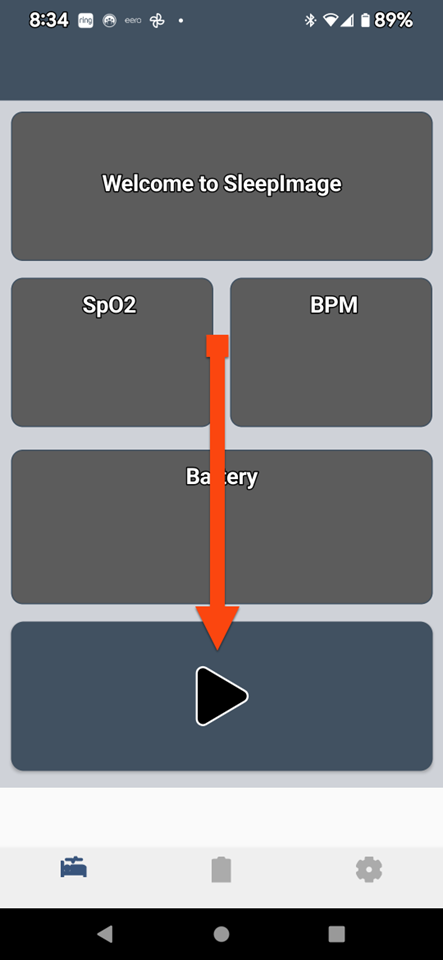
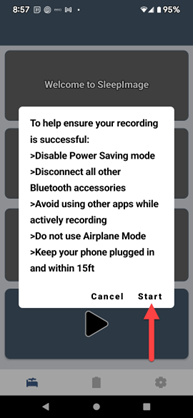
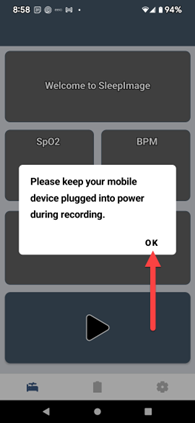
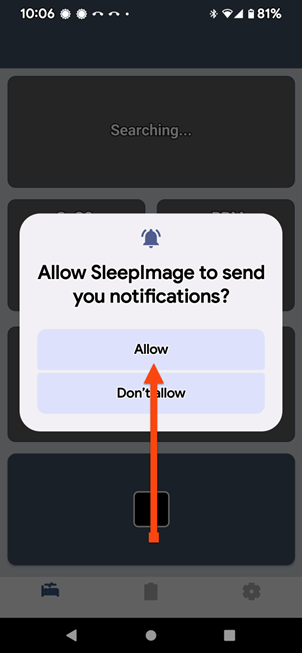
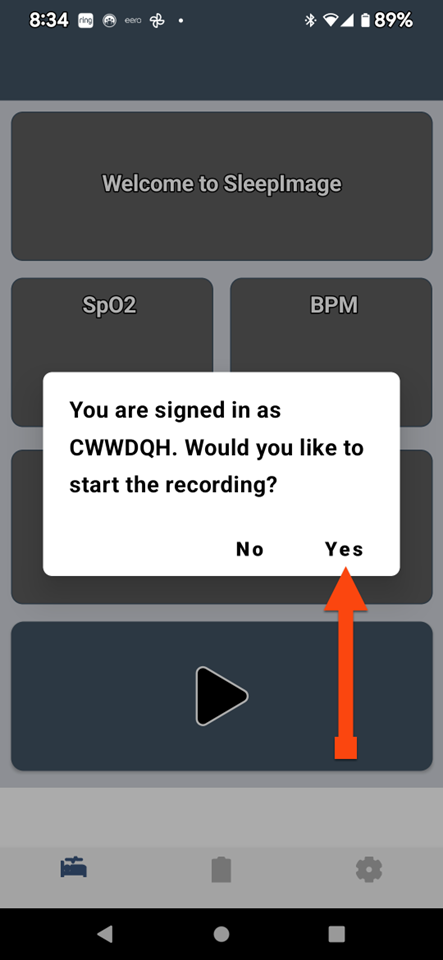
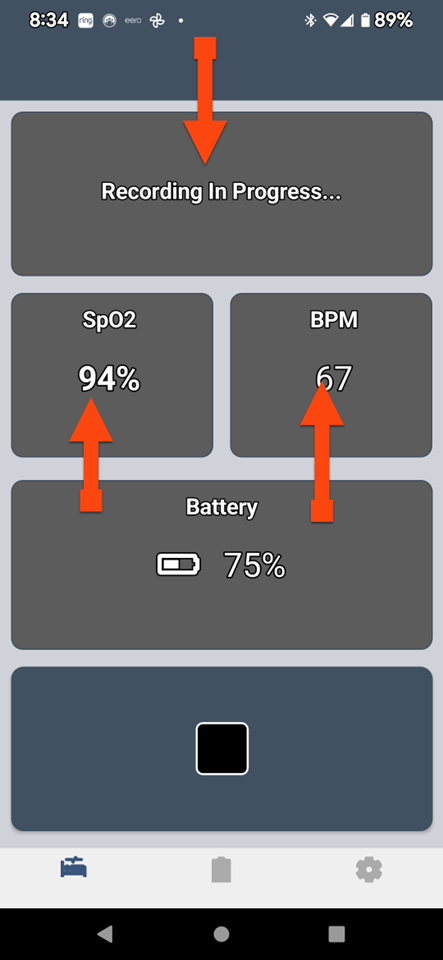
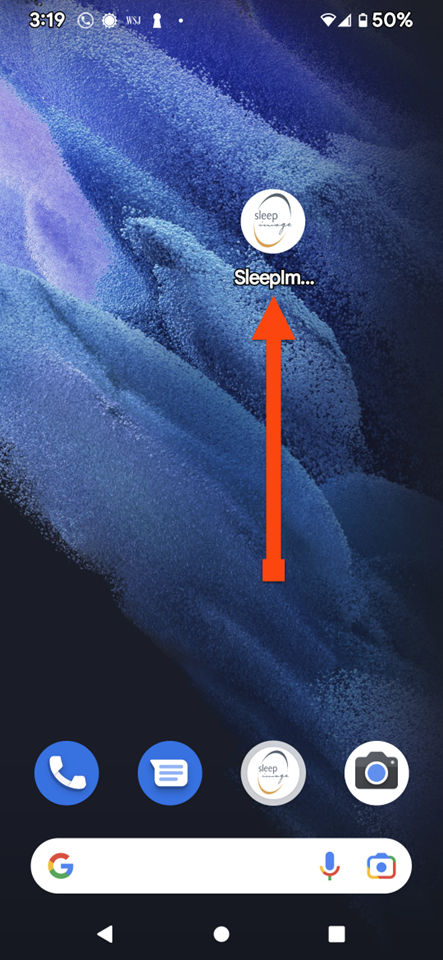
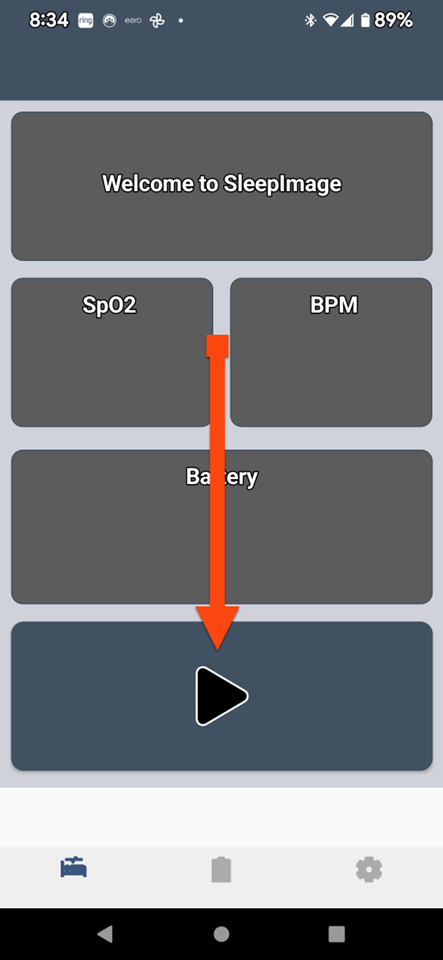
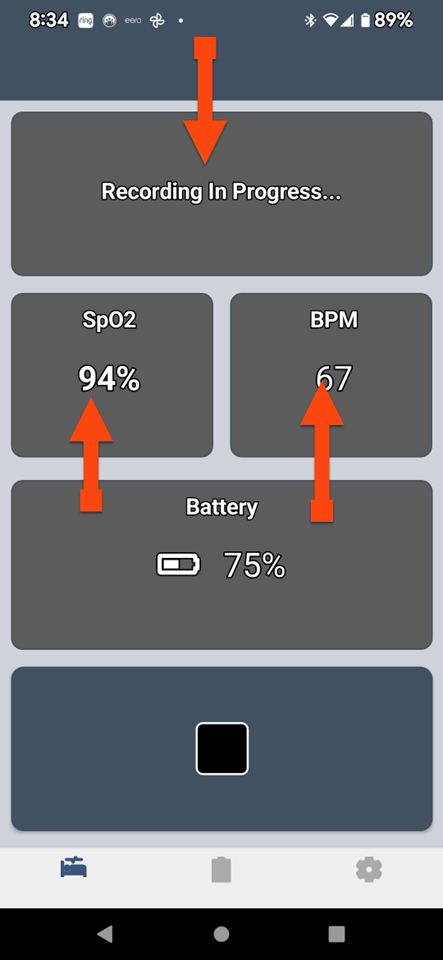
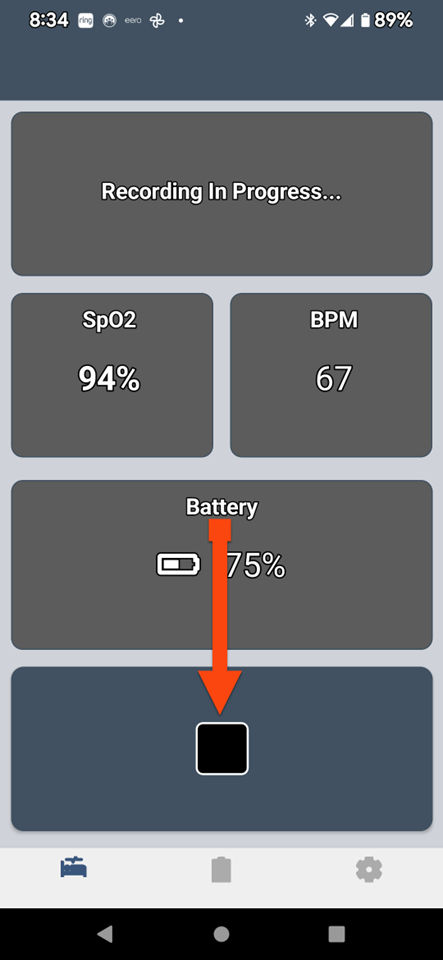
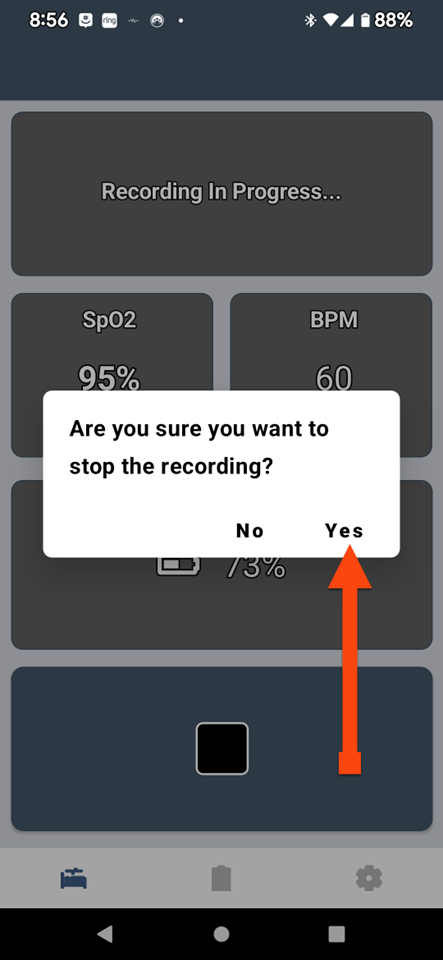
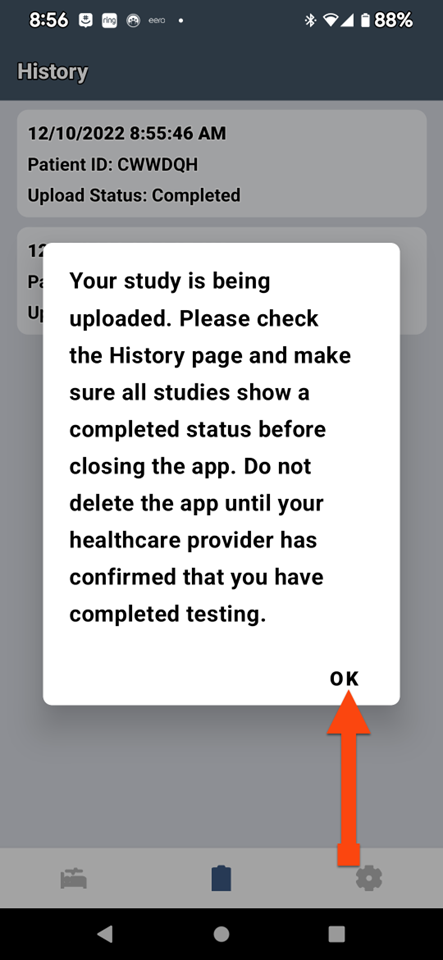
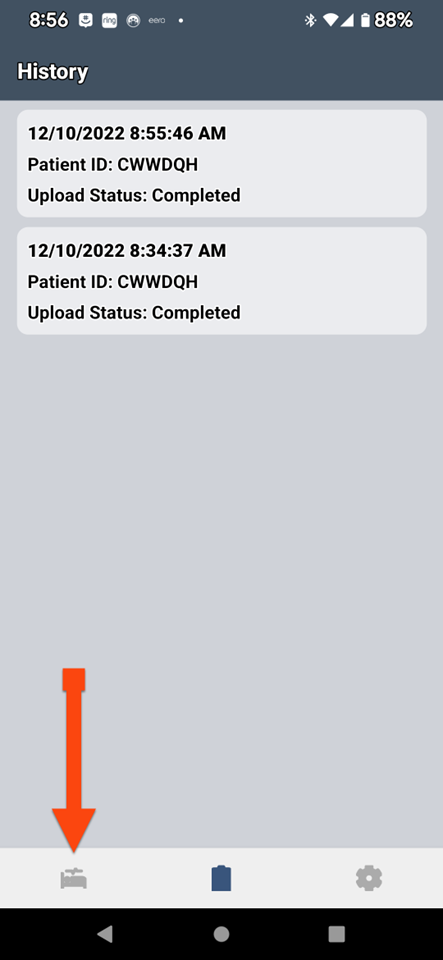
SLEEPIMAGE APP (Android)
WIFI vs. CELLULAR
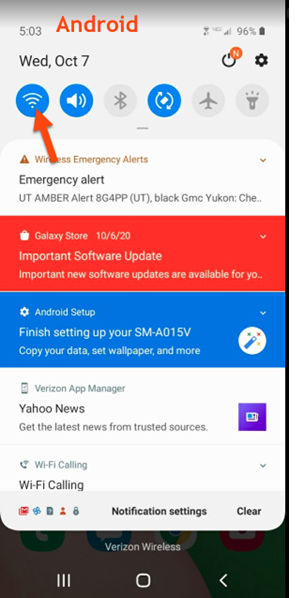
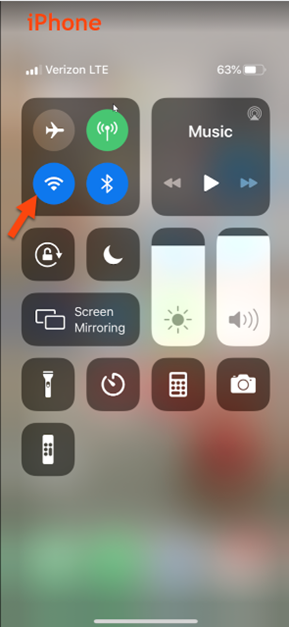
WIFI vs. CELLULAR

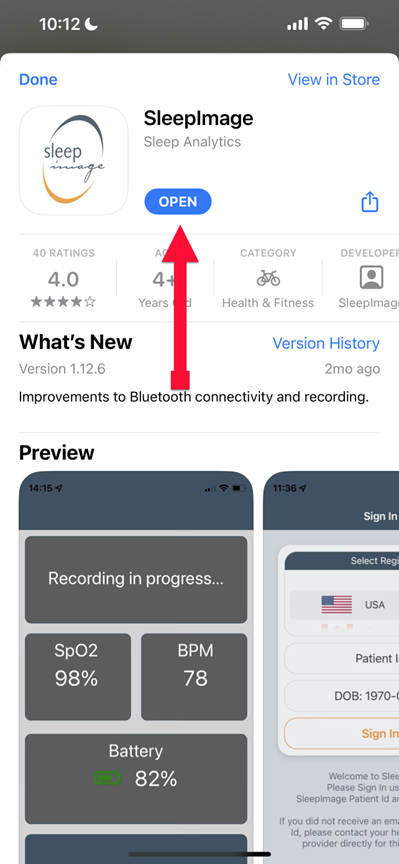
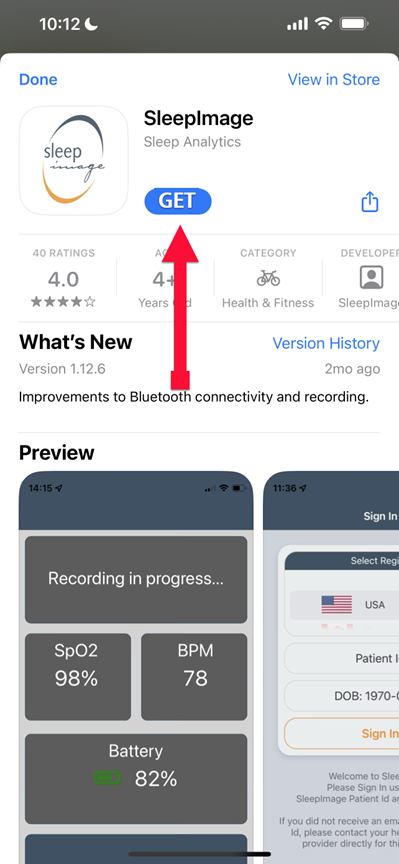
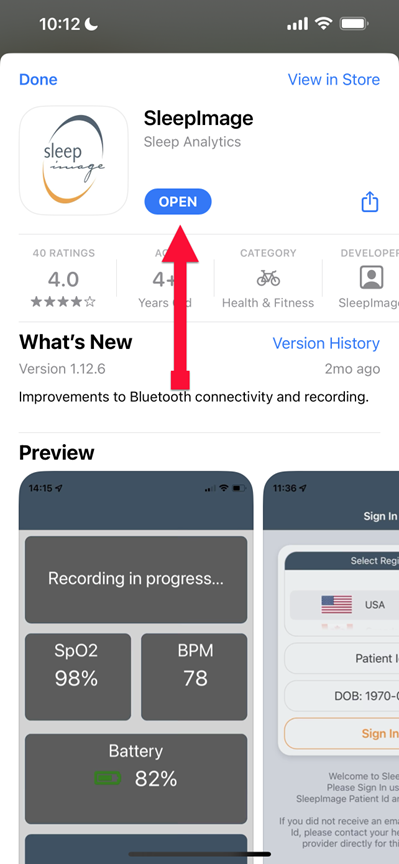
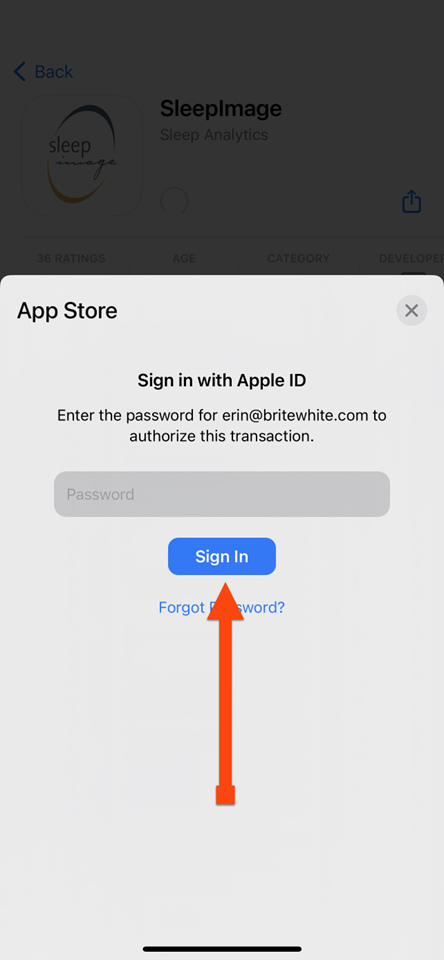
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)

SLEEPIMAGE APP (Android)

SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)

SLEEPIMAGE APP (iPhone)

SLEEPIMAGE APP (iPhone)
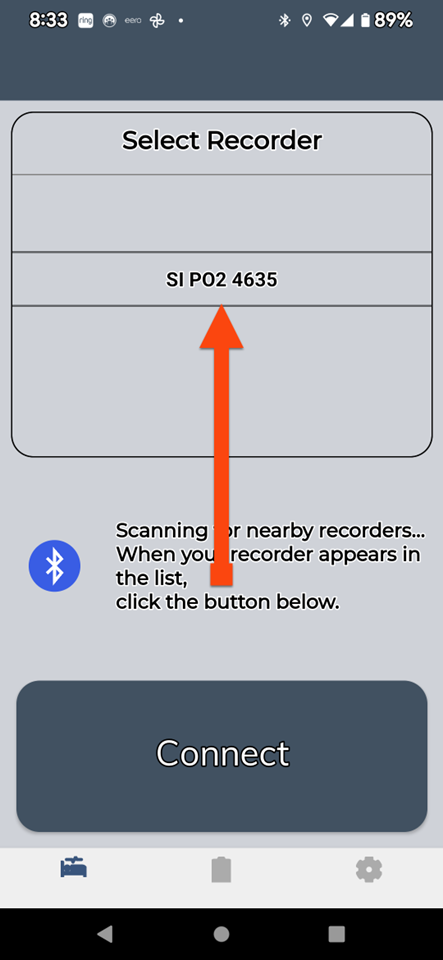
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)

SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)

SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (iPhone)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (Android)
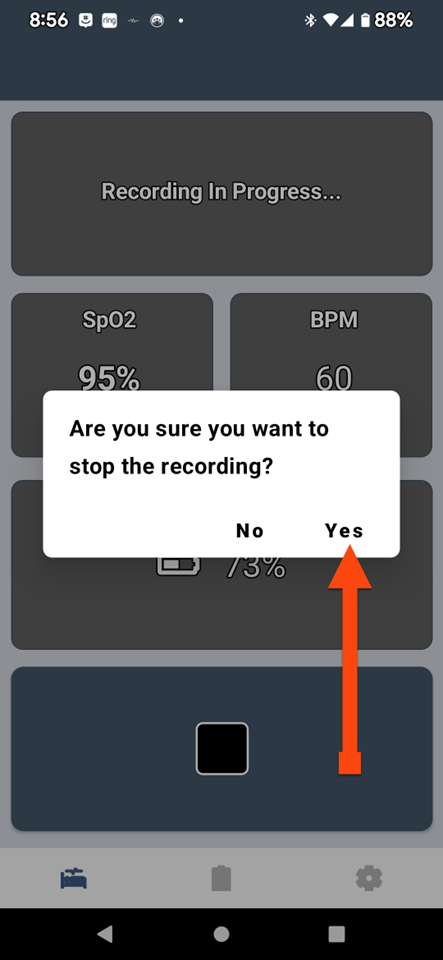
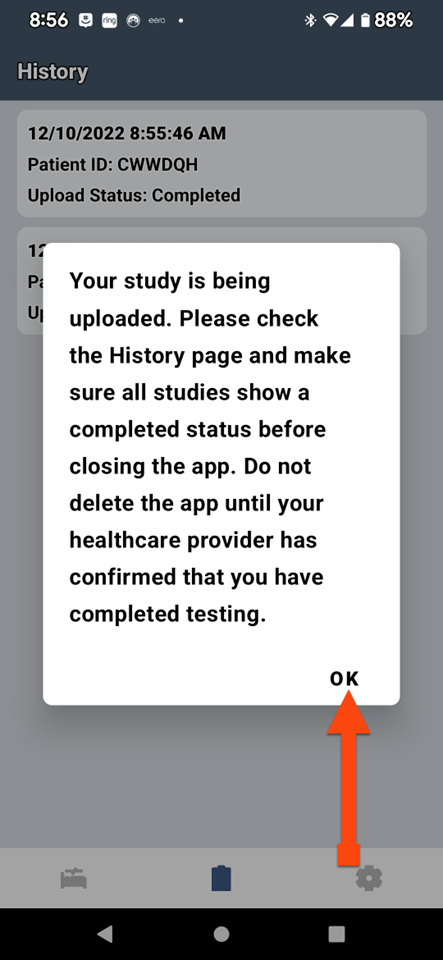
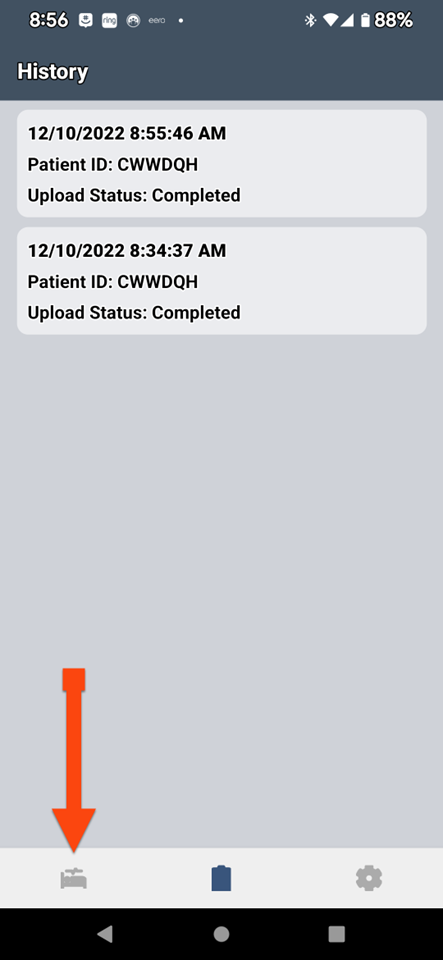
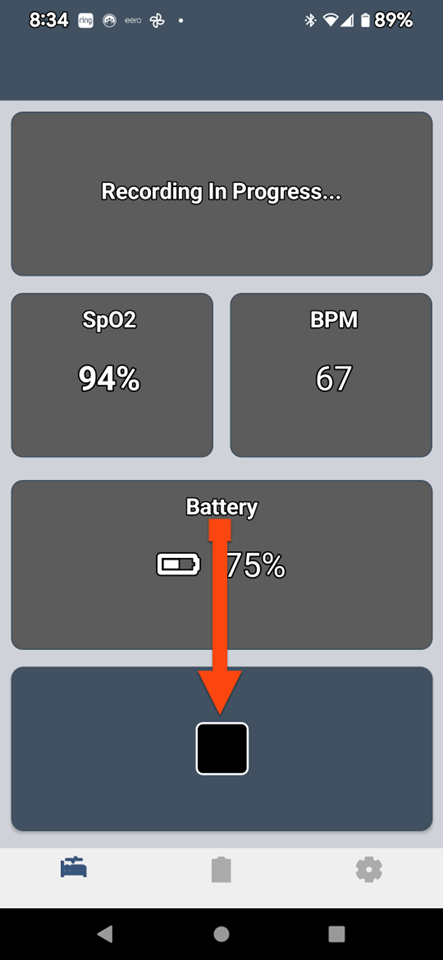
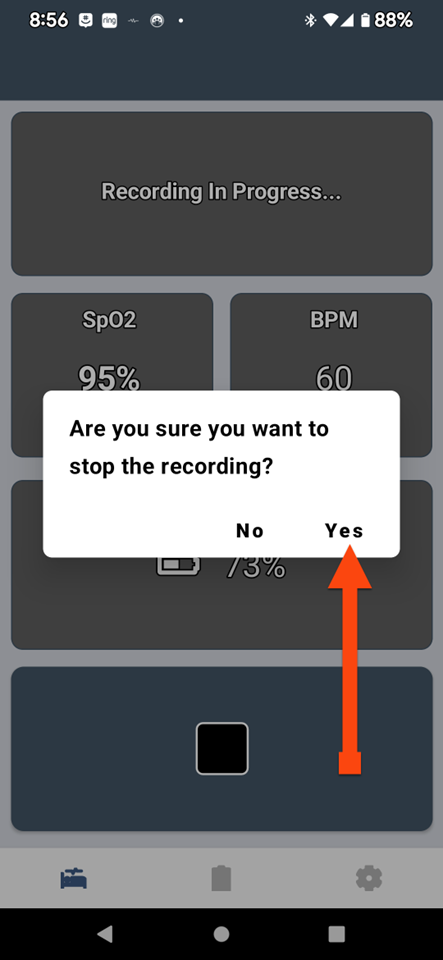
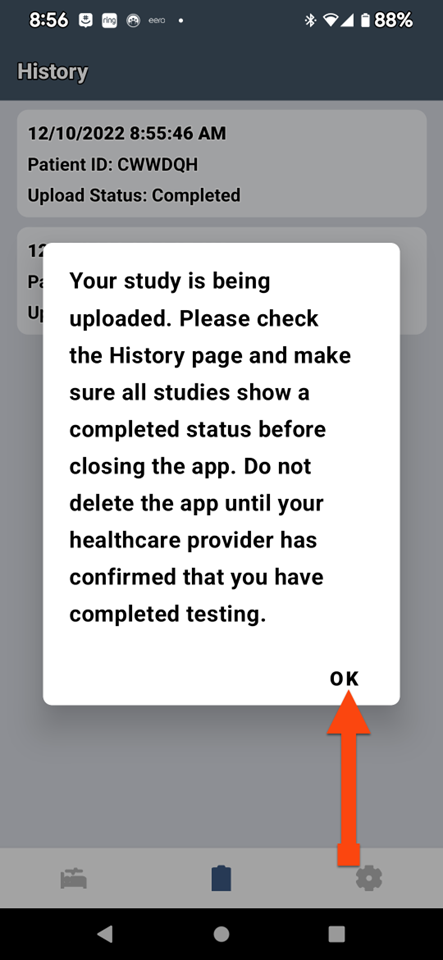
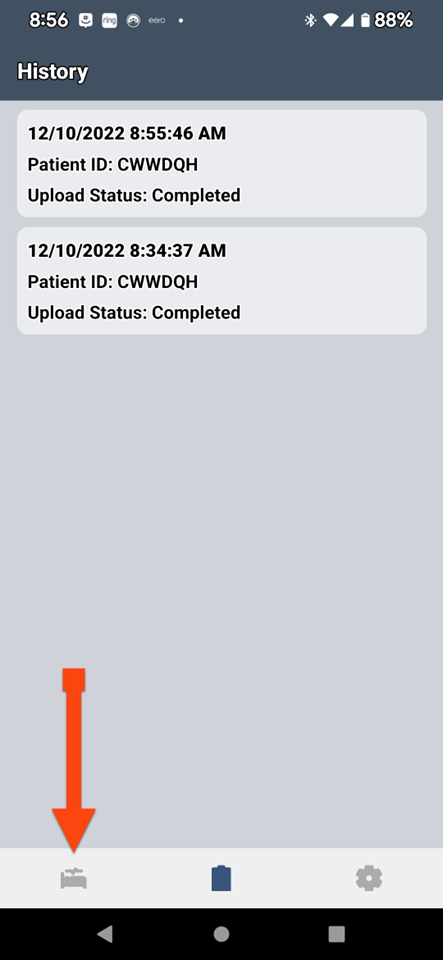
SLEEP TEST PROCEDURES

SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES
SLEEPIMAGE APP (Android)
SLEEPIMAGE APP (iPhone)
SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES

SLEEP TEST PROCEDURES

SLEEP TEST PROCEDURES
SLEEP TEST PROCEDURES
STOP BANG RESULTS
Stop Bang Results:
The Doctor will be with you shortly.
Keep the ASD Connect App Open
Intake & Assessment
What present illness do you have?
Intake & Assessment
What medications are you on?

Intake & Assessment
Do you experience any of the following?
- Excessive daytime sleepiness, tired or fatigued.
- Snores.
- Morning headaches.
- Difficulty falling or maintaining sleep.
- Irregular breathing during sleep.
- Bruxism.
- Witnessed apneas, gasping, or choking.
Intake & Assessment
Do you experience any of the following?
-
Impaired cognition.
-
Mood Disorder.
-
Insomnia.
-
Hypertension.
-
Ischemic heart disease.
-
History of strokes.
-
Excessive daytime sleepiness, tired, or fatigued.
Intake & Assessment
Have you ever used a CPAP?

Intake & Assessment
Can you tolerate your CPAP?
Intake & Assessment
Which of these reasons make you intolerant to your CPAP?
1. Claustrophobic.
2. Nonrestorative sleep.
3. Sinus infection (issues).
4. Facial Lesions.
5. Anxiety.
6. Mask fit issues.
7. Skin irritation or marks.
8. Mask leakage or Air leaking.
9. Dry mouth and nose.
10. Congestion.
11. Bloating (gas).
12. Excess phlegm.
13. Discomfort.
14. Rashes.
15. Aerophagia - swallowing air.
16. Nose bleeds.
17. Lung infections – Discomfort.
18. Headaches.
19. Dizziness.
20. Shortness of breath
Intake & Assessment
Stop Bang Results:
Intake & Assessment
Perform your sleep study this evening.
Intake & Assessment
Intake & Assessment
Present Illnesses
Medications
Sleep Complaints
Excessive Symptoms
CNT / Contraindicated
Which of these reasons are you contraindicated to using a CPAP?
1. Claustrophobic.
2. PTSD.
3. Sinus Infections (issues).
4. Anxiety.
5. Dry mouth or nose.
6. Nose bleeds.
7. Lung discomfort / infections
8. Facial deformity.
9. Vomiting.
10. Recent facial, neurological, or gastric surgery.
11. Chest, head or face trauma.
12. Paralysis
Intake & Assessment
APPOINTMENT DATE & TIME
Date:
Time:
Do you have cosmetic or restorative work done?
Intake & Assessment

How many teeth are you missing?
Intake & Assessment

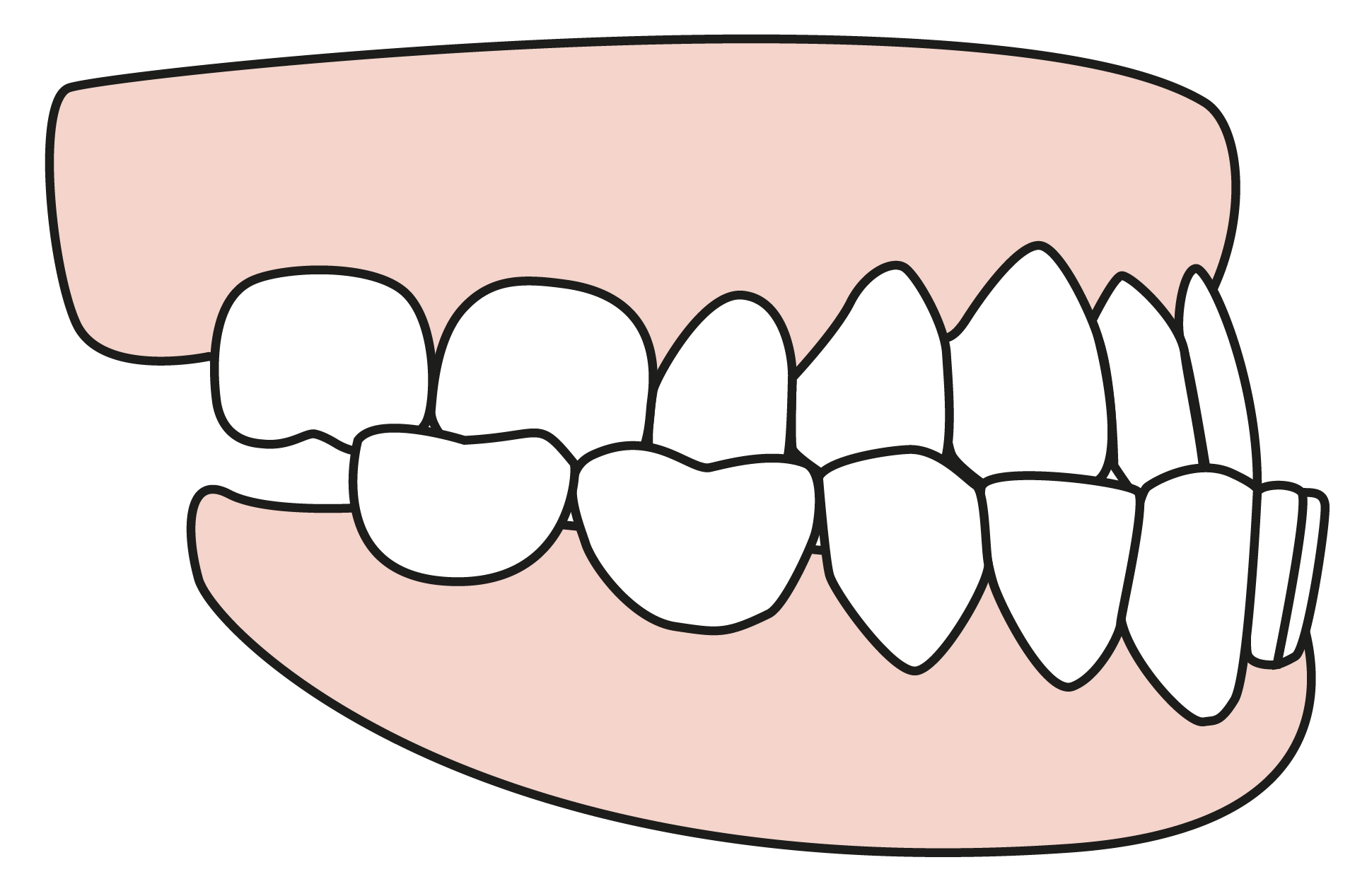
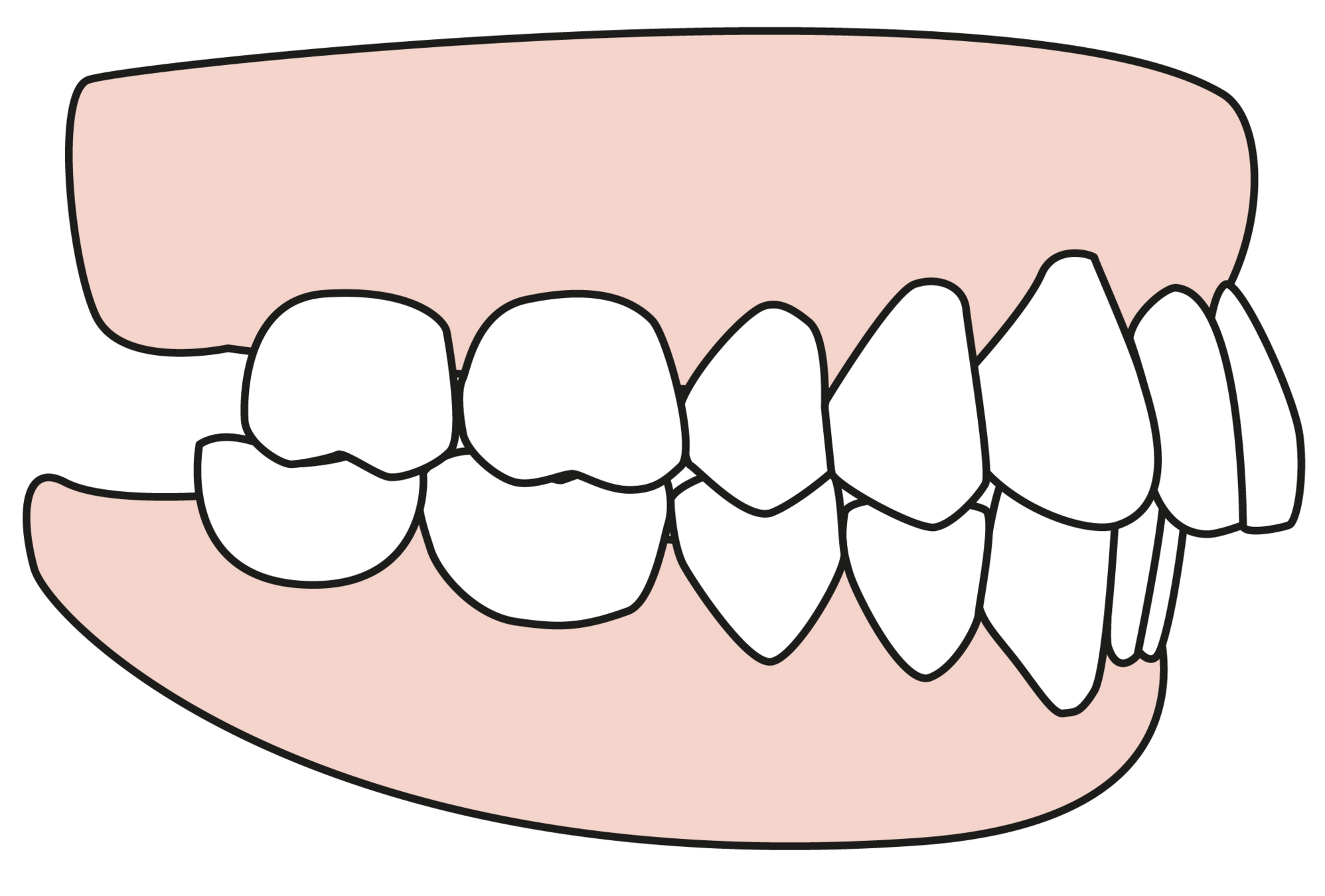
Do you an overbite or underbite?
Intake & Assessment
Do you have tooth decay?
Intake & Assessment

Do you have periodontal disease?
Intake & Assessment

Do you have bruxism?
Intake & Assessment

Do you have TMJ?
Intake & Assessment
Do you have allergies to acrylic or stainless steel?
Intake & Assessment

Intake & Assessment
Dental Work
Bite Type
Teeth Decay
Periodontal Disease
Bruxism
TMJ
Allergies
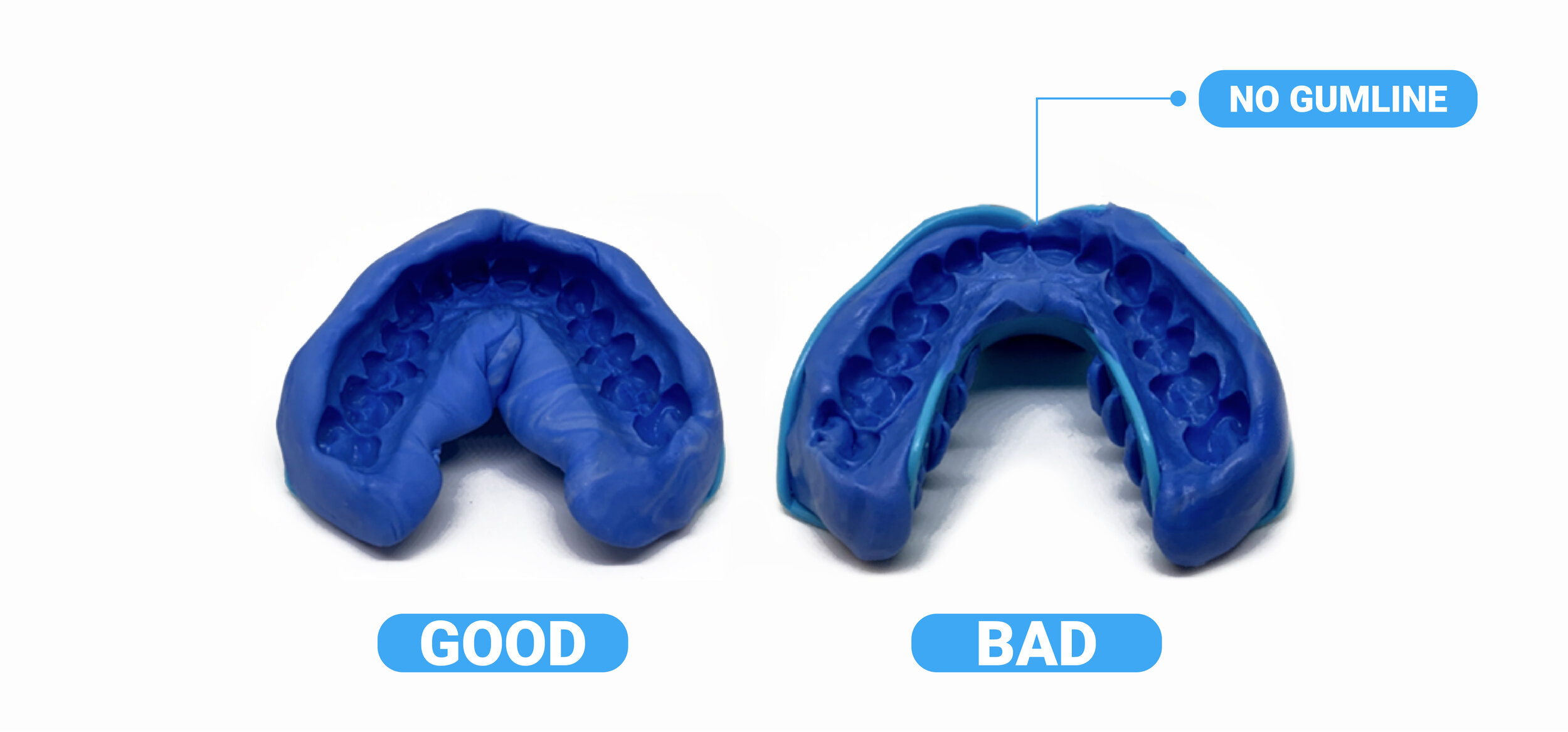
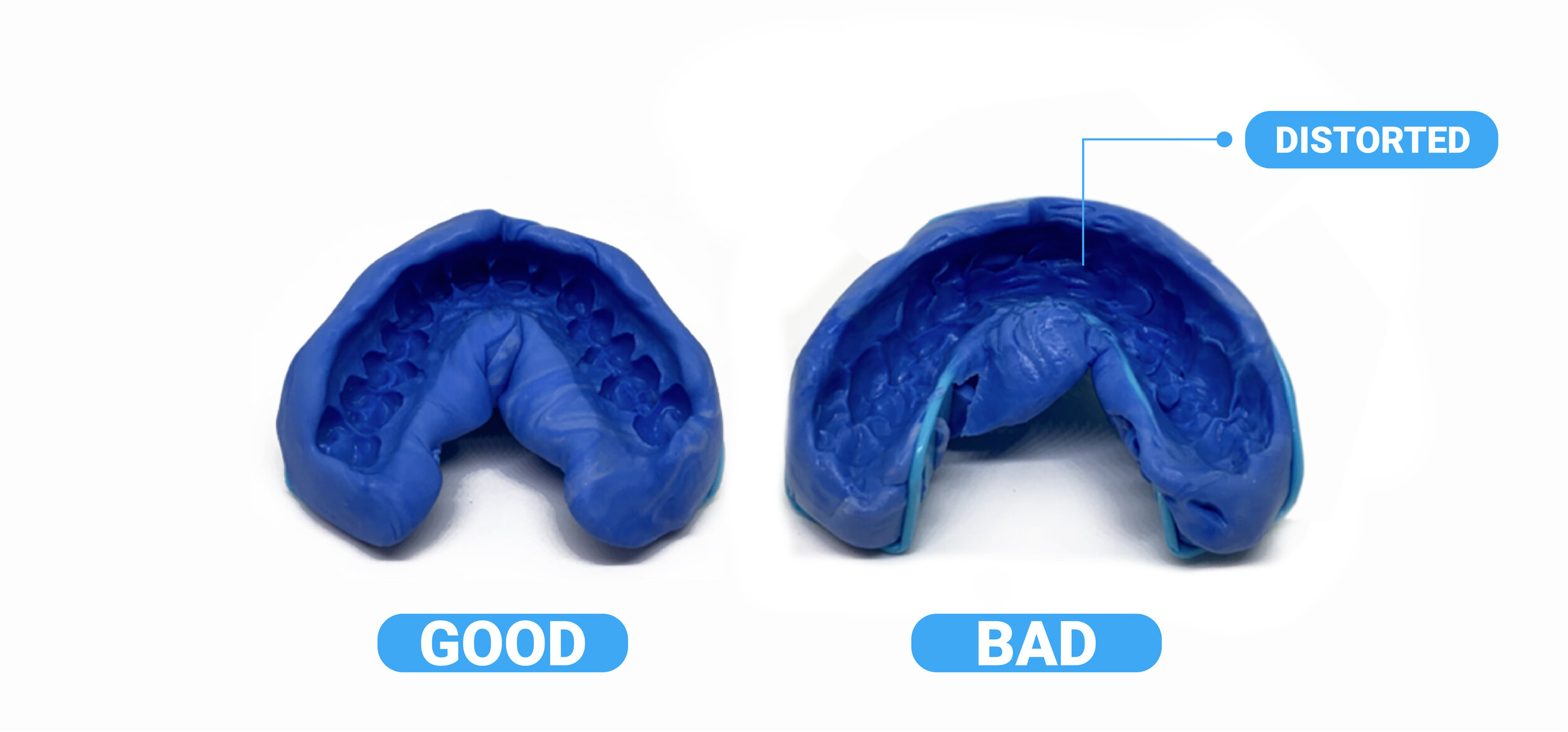
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions
Taking Impressions

Text
Taking Impressions
Text
Taking Impressions

Taking Impressions
Complete Form
Placing Impression
APPOINTMENT DATE & TIME
APPOINTMENT DATE & TIME
Date:
Time:
RELEASE & AUTHORIZATION
I, , hereby acknowledge:
- Dentist and American Sleep Dentistry only guarantees that which is in writing (no implied guarantees and does not guarantee against tooth sensitivity, movement of teeth, damaged teeth, and teeth problems.
- Dentist and ASD are acting according to the treatment plan and order of your medical doctor. Dentist and ASD legally cannot create or alter a treatment plan or order for the treatment of OSA. Only a medical doctor can.
- By signing, patient represents that they have reviewed and agree to the 'Terms & Conditions' found at www.americansleepdentistry.com.
- Patient agrees that ASD can process the patient's credit card on file for their deductible and coinsurance.
- Patient agrees that the total liability is limited to the amount of the product.
, do you agree with what I have just read? [Yes.] If you had a paper document, you would confirm that you agree by signing your name. In this conversation, you can confirm that you agree by saying your first and last name. If you say your name, it is the same as if you were signing a piece of paper. If you agree and intend to sign these agreements, please say your first and last name.
Stay Online. We will be with you shortly!
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Fitting Sleep Appliance
Warranty

RELEASE & AUTHORIZATION
I, , hereby acknowledge that on :
- The Dentist fitted and adjusted the oral appliance.
- The Dentist explained how to care for the oral appliance.
- The Dentist advised me to continue to working with my medical doctor and my normal dentist.
- I have reviewed and agree to the 'Terms & Conditions' found at www.americansleepdentistry.com/terms.html.
- I agree that the total liability is limited to the amount of the product.
- The Dentist and ASD are acting according to the treatment plan and order of my medical doctor. Dentist and ASD legally cannot create or alter a treatment plan or order for the treatment of OSA. Only a medical doctor can.
Review
On a scale of 1-10 how would you rank our services ?
Needs Work
Good Work
Google Review

Connecting Doctor
The Dentist will be with you shortly.
Keep the ASD Connect App Open
APPOINTMENT DATE & TIME
APPOINTMENT DATE & TIME
Date:
Time:
Intake & Assessment
Dental Work
Dentures
Bite
Teeth Decay
Periodontal Disease
Bruxism
TMJ
Allergies